ОРВИ, простуда, кашель, боль в горле и заложенный нос – состояние, которое сложно переносить и взрослому человеку, не говоря уже о ребенке. Одним из эффективных способов лечения вирусных заболеваний и облегчения их симптомов является небулайзерная терапия. Ингаляции для детей – это эффективно, быстро и безболезненно: часто ребенок охотнее согласится «посидеть» 5 минут с небулайзером, чем принимать невкусное лекарство. Использование ингалятора будет полезно на различных стадиях заболевания: прибор преобразует лекарственное средство в мельчайшие частички (аэрозоль), способные проникать непосредственно к месту локализации болезни, будь то бронхи или легкие. Именно это точечное воздействие и делает ингаляции такими эффективными в лечении детей.
Максимально удобным в использовании станет именно меш-небулайзер (электронно-сетчатый), ведь он обладает рядом неоспоримых преимуществ перед другими типами приборов (компрессорными, ультразвуковыми, паровыми):
- меш-небулайзер не разрушает никакие лекарственные средства в процессе работы (например, многие действенные растворы не совместимы с ультразвуковыми приборами именно по этой причине);
- ингаляторы этого типа можно применять со всеми лекарствами, кроме созданных на масляной основе (причина этому не только технологическая особенность прибора, но и безопасность – масляные растворы опасны для ингаляций и имеют ряд весьма серьезных противопоказаний);
- эти приборы работают бесшумно, не пугают и не раздражают ребенка – в момент плохого самочувствия дети особенно чувствительны к раздражителям;
- меш-небулайзер имеет небольшие размеры, может работать как от батареек, так и от сети – прибор всегда можно взять с собой при необходимости или просто проводить ингаляцию с комфортом дома, расположившись удобно.

Врач-пульмонолог, аллерголог-иммунолог
Задать вопрос
Врач-пульманолог, аллерголог-иммунолог. Стаж: 38 лет. Образование: в 1982 году окончила лечебный факультет Рязанского медицинского института им. И.П. Павлова, там же в 1983 году — интернатуру.
Содержание
- Как правильно проводить ингаляцию для детей небулайзером?
- Ингаляции при кашле у детей – особенности.
- Ингаляции при насморке у детей – особенности.
- Ингаляции для профилактики простуды и ОРВИ: эффективно ли?
- Ингаляционная терапия: показания и противопоказания
- Виды ингаляций
- Разновидности аппаратов и принцип их действия
- Как проводить ингаляции
- Ошибки при использовании ингалятора
- Показания к применению
- Лечебный эффект ингаляции
- Противопоказания к физиопроцедуре
- Побочное действие
- Ингаляция в домашних условиях
- Ингаляция для детей
- Что заливать в ингалятор
- Лекарства для небулайзера
- Эфирные масла
- Физраствор
- Заключение
- Как вылечить насморк. Препараты от насморка
- Что такое ринит?
- Современные препараты для лечения насморка
- Капли и спреи от насморка
- Таблетки от насморка
- Мази от насморка
- Масла от насморка
- Ингаляции при насморке
- Как правильно выбрать средство от ринита
- Ринит у беременных
- Определение и понятие
- Встречаемость
- Причины и механизм возникновения
- Прогрессирование и потенциальные риски
- Диагностика
- Выбор лечебной тактики
- Доктор, не помогает.
- Кто такие FDA в США и почему их все слушают?
- Да не буду я принимать эти гормоны!
- Физраствор – универсальное лекарство
- Натрия хлорид – что это?
- Когда используют
- Способы применения
- Подкожное и внутривенное введение
- Для промывания носоглотки
- Для очищения желудка и кишечника
- Противопоказания и побочные реакции
- Ингаляционная терапия: показания и противопоказания
- Виды ингаляций
- Разновидности аппаратов и принцип их действия
- Как проводить ингаляции
- Ошибки при использовании ингалятора
- Показания к применению
- Лечебный эффект ингаляции
- Противопоказания к физиопроцедуре
- Побочное действие
- Ингаляция в домашних условиях
- Ингаляция для детей
- Что заливать в ингалятор
- Лекарства для небулайзера
- Эфирные масла
- Физраствор
- Заключение
Как правильно проводить ингаляцию для детей небулайзером?
- Перед началом ингаляции для ребенка обязательно изучите инструкцию по применению конкретно вашего прибора, там могут быть важные нюансы.
- Помните, что грамотную схему лечения, конкретное лекарство и дозировки может назначить только врач.
- Для проведения ингаляции используйте только предназначенные для этого лекарственные средства, не используйте кипяченую и дистиллированную воду — это не только не будет эффективным, но и может стать опасным и привести к бронхоспазму. Что касается использования минеральной воды без газа для ингаляций – она может применяться, но только по назначению врача, например, когда у ребенка есть небольшое количество вязкой мокроты в дыхательных путях (кашель с трудноотделяемой мокротой). Вместе с тем, использование минеральной воды может вызвать раздражение задней стенки глотки, а также спровоцировать уже упомянутый выше бронхоспазм.
Также не используйте эфирные масла, настои или отвары трав.
- Распространенным является вопрос, можно ли проводить ингаляции при температуре ребенку. Зависит от температуры, но скорее нет, чем да. Врачи не рекомендуют делать ингаляции ребенку при температуре выше 37, 5 градусов.
- Не проводите ингаляции сразу после еды или после активных игр, любой иной физической активности.
- Лекарство, которое хранится в холодильнике, перед использованием следует достать и дать ему немного нагреться.
- Если на одежде ребенка есть какие-то элементы, которые мешают ему свободно дышать – снимите их. Дыхание должно быть свободным.
- После того, как ингаляция окончена – проведите очистку прибора, всех деталей и высушите их.
Вопросы о том, какие делать ингаляции ребенку, рецепты ингаляций, сколько минут делать ингаляции, сколько дней или сколько раз в день – все это план лечения, который назначит педиатр. Только специалист после осмотра ребенка и расшифровки анализов может дать вам ответы на эти вопросы. Самолечение может быть неэффективным и даже опасным.
Ингаляции при кашле у детей – особенности.
Важно понимать, какой у ребенка кашель – влажный или сухой, от этого будет зависеть, какое именно лекарство выбрать для ингаляции. При борьбе с кашлем ингаляция осуществляется так: вдох производится через рот, выдох через нос.
Ингаляции при сухом кашле у ребенка прежде всего нацелены на то, чтобы увлажнить слизистые оболочки, сделать мокроту более жидкой. Для этого врачи назначают муколитики, бронхолитики и/или противовоспалительные средства. На начальном этапе болезни может быть достаточно ингаляции с физраствором (к вопросу о том, можно ли физраствором делать ингаляции детям — ответ «да», но по назначению).
При влажном кашле ингаляции имеют другую направленность: оказать отхаркивающее, дезинфицирующее и антисептическое действие. Таким образом мокрота будет выводиться из легких быстрее.
Ингаляции при насморке у детей – особенности.
При насморке, болезнях носовой полости ингаляции проводятся следующим образом: вдох и выдох производятся строго через нос. Для лечения могут использоваться такие средства, как синупрет, хлорфиллипт, мирамистин, ротокан, ринофлуимуцил и другие (конкретное средство и дозировки назначает врач, в зависимости от тяжести болезни; названия лекарственных средств приведены для примера и не являются рекомендацией к лечению).
В каких случаях при насморке нельзя проводить ингаляцию:
- у ребенка болят уши, есть подозрения на отит;
- слизь из носа имеет зеленоватый или желтоватый оттенок, это может свидетельствовать о развитии бактериальной инфекции, и в таком случае ингаляции могут вызвать осложнения;
- у ребенка есть предрасположенность к носовым или легочным кровотечениям.
Ингаляции для профилактики простуды и ОРВИ: эффективно ли?
Наиболее эффективным для профилактики ОРВИ все же является правильное и разнообразное питание, прием витаминов и минералов, режим сна, достаточный уровень физической активности. Однако ингаляции с физраствором могут также помочь в профилактике в периоды сезонного подъёма заболеваемости. Рекомендуется приобретать физиологический раствор в аптеке, а не готовить самостоятельно.
Ингаляции – это эффективный и простой способ помочь ребенку справиться с ОРВИ, простудой, кашлем и насморком. Для того, чтобы процедура прошла безопасно и комфортно, и принесла только положительный результат, выбирайте правильный меш-небулайзер для домашнего использования и применяйте в лечение лекарственные средства, назначенные врачом. Будьте здоровы!
Ингаляционная терапия: показания и противопоказания

Ингаляционная терапия – процедура при которой, пациент вдыхает лекарственные вещества или воздух через небулайзер. Процедура назначается как в лечебных целях, так и целях профилактики.
Цель ингаляционной терапии – доставить лекарственное вещество в определенную область дыхательных путей, при этом минимизировать накопление препарата в других органах.
Виды ингаляций
На практике применяются различные виды ингаляции, которые представлены далее:
- Паровые. Самый распространенный вид ингаляции при котором пациент вдыхает горячий пар. Процедура назначается при заболевании верхних дыхательных путей: фарингит и ринит, снимает отек.
- Тепловлажные используются с теплым воздухом и аэрозолями солей. Курс процедур способствует отхаркиванию и выведению слизи.
- Влажные разрешены тем, кому противопоказаны паровые и тепловлажные. Раствор распыляется в дыхательные пути без подогрева.
- Сухие. Воздух при таком сеансе сухой и горячий, подходит для лечения ОРЗ;
- Воздушные. Воздух распыляется с помощью баллончика, обладает бронхолитическими свойствами;
- Масляные ингаляции основаны на распылении подогретых масел, которые подходят при сухости и покрывают защитной плёнкой органы дыхания;
- Ультразвуковые ускоряют выздоровления и способствуют отхаркивания. На лекарство аппарат воздействует ультразвуком.
Разновидности аппаратов и принцип их действия
Ингаляторы разделяются на 4 вида:
1. Паровые – приборы которые нагревают вещество до газообразного состояния. При использовании данного ингалятора частицы попадают в верхние дыхательные пути.
2. Компрессорные ингаляторы. Принцип действия заключается в нагнетании воздуха под давлением при помощи компрессора.
3. Ультразвуковые – аппараты которые воздействуют ультразвуком на вещество, превращая его в аэрозоль.
4. Меш-ингаляторы. Лекарство проходит через сетку с отверстиями, создавая при этом аэрозоль.
Подобрать подходящий ингалятор поможет врач, исходя из цели процедуры.
Как проводить ингаляции
1. Прекратить приём пищи и физических нагрузок за 2 часа до сеанса;
2. Перед началом ингаляционной терапии заливается лекарство;
3. Сеанс проходит в положении сидя в расслабленном состоянии;
4. Включите ингалятор;
5. Мундштук прибора плотно обхватите губами;
6. Во время ингаляции вдыхайте полной грудью и медленно;
Длительность сеанса и лекарственные препараты назначаются исходя из диагноза лечащим врачом.
Ошибки при использовании ингалятора
Наиболее распространённые ошибки при проведении физиопроцедуры:
1. Не обрабатывать аппарат. Даже при использовании прибора одним человеком, обязательно проводить обработку ингалятора.
2. Заливать раствор в прибор, не имея представления о том, что можно применять, а что нет.
3. Проводить процедуру имея противопоказания.
4. Использовать аппарат сразу после больного.
5. Не соблюдать время проведения сеанса, назначенного врачом.
Показания к применению
- Заболевания верхних дыхательных путей (легких и бронхов);
- Бронхиальная астма;
- Заболевания среднего уха;
- Аллергический ринит;
- Профилактика простудных заболеваний;
- Остаточные явления пневмонии;
- Грипп;
- ОРВИ;
Лечебный эффект ингаляции
- Способствует выведению мокроты;
- Снимает напряжение;
- Уменьшает воспаления;
- Борется с микробами;
- Укрепляет иммунитет;
- Снимает спазм бронхов;
Противопоказания к физиопроцедуре
При всей пользе от терапии существует ряд противопоказаний, которые необходимо учитывать:
- Аллергия на применяемые растворы или его компоненты;
- Расширение альвеол легких в тяжелой форме;
- Кровотечение из носа;
- Повышенная температура тела;
- Дыхательная недостаточность;
- Заболевания сердца;
Побочное действие
При глубоком вдохе возможно головокружение и тошнота, появление кашля. Процедура безопасна, побочные эффекты могут возникнуть при наличии противопоказаний и не соблюдении рекомендаций специалиста.
Ингаляция в домашних условиях
Физиопроцедура в домашних условиях эффективно дополнит лечение простудных заболеваний, борется с кашлем и способствует выведению мокроты. Сегодня не составит труда приобрести небулайзер.
Рекомендации для ингаляции в домашних условиях:
- Не принимать пищу за 1.5 часа до сеанса;
- Если лекарство вы используете впервые, то вдыхание стоит проводить не более 2 минут, на случай выявления аллергии на препарат или активные компоненты;
- Не разговаривать в процессе ингаляции;
- После процедуры следует расслабиться и полежать 20-30 минут;
Ингаляции при помощи небулайзера безопасны и просты в применении. Процедуру в домашних условиях можно сделать с применением минеральной воды или с использованием эфирных масел.
Минеральная вода способствует выведению и разжижению мокроты.
Эфирные масла смягчают слизистую и облегчают дыхание.

Ингаляция для детей
Ингаляцию для ребёнка можно проводить с 2 лет, но только по рекомендации врача. Паровые ингаляции запрещены.
1. Проводите процедуру каждый день в одно и тоже время, чтобы ребёнок привык.
2. Отвлеките ребёнка: читать книжку, дать игрушку или включить любимые мультики.
3. Если ребёнок вел себя спокойно и соблюдал все правила, похвалите его в конце.
Что заливать в ингалятор
В зависимости от того, какую цель преследует ингаляция препарат подбирается индивидуально. Вдыхание веществ намного эффективнее чем прием таблеток, так как активные компоненты действую локально. Однако не стоит пренебрегать лечением. В небулайзер заливают такие растворы как: эфирные масла, физрастворы и лекарства.
Лекарства для небулайзера
Препарат и его дозировка назначаются только лечащим врачом, не стоит заниматься самолечением. Существует 5 групп, которые используются при физиопроцедуре.
- Бронхолитики используют для лечения бронхиальной астмы и хронического заболевания лёгких.
- Нестероидные противовоспалительные препараты — снимают болевые ощущения и воспаления, применяются при лихорадке.
- Антибиотики назначают при бактериальных инфекциях.
- Кортикостероиды — стероидные средства, которые эффективны в борьбе с воспалительными процессами.
- Муколитики — разжижают мокроту и способствуют выведению слизи из лёгких.
Эфирные масла
Жидкость, которую можно заливать только в паровые ингаляторы. Масла доказывают свою эффективность при профилактике гриппа и ОРВИ. Чаще остальных применяют масла эвкалипта, чайного дерева и аниса.
Физраствор
Физраствор – жидкость, которая состоит из воды и натрий хлора 0,9%. Данное соединение безопасно и подходит даже для ребёнка. Аналог раствора можно сделать в домашних условиях из дистиллированной воды и поваренной соли. Состав ускоряет выведение мокроты и смягчает слизистую. Минеральная вода боржоми считается аналогом физраствора.
Заключение
Ингаляционная терапия пользуется популярностью среди физиопроцедур и решает ряд проблем, выступает в целях профилактики и лечения заболеваний дыхательных путей. Процедура безопасна для пациентов любых возрастов. Вдыхание лекарственных веществ при помощи пара приобретает особую значимость при лечении органов дыхания.
Как вылечить насморк. Препараты от насморка
Как избавиться от насморка быстро и без последствий для организма? Для этого следует выяснить причину появления негативной симптоматики, определив вид ринита (простудный, аллергический, инфекционный и пр.) и грамотно подобрать лекарства.
Как избавиться от насморка быстро и без последствий для организма? Для этого следует выяснить причину появления негативной симптоматики, определив вид ринита (простудный, аллергический, инфекционный и пр.) и грамотно подобрать лекарства.
Что такое ринит?
Это воспаление слизистой оболочки носа. Болезнь имеет две стадии, каждая из которой сопровождается характерной симптоматикой. В некоторых случаях заболевание принимает затяжное течение и тогда речь идет о хронической форме заболевания.

при первых признаках болезни следует обязательно принимать лекарства от ринита.
В противном случае болезнь может привести к серьезным осложнениям и перейти в хроническую форму, сложно поддающуюся терапии. Кроме того, люди с сильным насморком, с чиханием и соплями продолжают посещать места общего пользования ездить в транспорте и ходить на работу, подвергая опасности инфицирования окружающих.
Насморк чрезвычайно заразен! Особенно легко заражаются маленькие дети, пожилые люди и пациенты с ослабленным иммунитетом.

Внимание! Не следует использовать никакие народные методы от насморка! В тех случаях, когда насморком заболел малыш, пожилой человек или пациент, страдающий любыми тяжелыми хроническими заболеваниями, лечение проводят только после консультации с врачом. Так, при многих формах насморка подобное «бабушкино» лечение приводит к значительному ухудшению состояния. Например, при закапывании сока лука или чеснока происходит сильное раздражение и без того воспаленной слизистой оболочки. Она разбухает еще больше, чихание усиливается, носовое дыхание ухудшается.
Как лечить насморк, чтобы не допустить осложнений и перехода заболевания в хроническую форму? Современная медицина предлагает множество лекарственных средств – это действенные препараты от насморка любого вида.
Современные препараты для лечения насморка

Капли и спреи от насморка
Капли от насморка и спреи – наиболее популярные и удобные в применении лекарственные формы. Они устраняют сухость и заложенность, снимают воспаление, улучшают благодаря восстановлению носового дыхания общее состояние больного. Данные лекарства могут включать в свой состав антибактериальные ингредиенты.
Название
Действие
Минусы
Примеры препаратов
Сосудосуживающее средство от насморка
Сужение сосудов, уменьшения отека, снятие заложенности, освобождение носового дыхания
Не действуют на воспалительный процесс
Не обладают лечебным эффектом
Симптомы снимаются лишь на время
Вызывают быстрое привыкание
Нельзя использовать в случае некоторых заболеваний – это гипертония, атеросклероз, аритмия, глаукома
Обладают внушительным списком побочных действий, это: головокружение, головная боль, повышение артериального давления, шум в голове и др.
Период действия – от трех до шести часов:
От шести до восьми часов:
От 10 до12 часов:
При густых/гнойных выделениях из носа
Имеют те же побочные действия, что и сосудосуживающие средства
увлажнение слизистых оболочек, разжижение слизи вхождение в состав морской воды позволяет эффективно очистить пазухи носа от болезнетворных вирусов, бактерий, а также аллергенов
Не оказывают мгновенного действия
Подходят для профилактики
Входят в состав комплексного лечения
Сосудосуживающее действие проявляется мягко
Очистка пазух носа от бактерий и вирусов
Эффект проявляется не сразу
Антибактериальное средство от насморка
Показания – бактерицидный ринит
густые желто-зеленые выделения из носовых пазух
В основном относятся к рецептурным лекарствам
Длительное и/или частое использование антибиотиков является следствием формирования устойчивых болезнетворных микроорганизмов (бактерий и пр.)
Таблетки от насморка
В ряде случаев есть смысл использовать другие формы лекарств от ринита. Как лечить насморк с помощью драже и таблеток?
Существуют растительные и гомеопатические препараты, которые практически не имеют противопоказаний и побочных действий в сравнении с некоторыми каплями. Препараты от насморка в виде таблеток, капсул, драже принимаются внутрь согласно инструкции. Если капли в основном убирают негативную симптоматику, таблетки могут быть на порядок эффективнее, так как действуют на причину заболевания.
Мази от насморка
Средство от насморка в виде мази – удобная форма лечения и профилактики многих видов ринита. Так же, как и другие лекарства мази бывают:
- противовирусные;
- гомеопатические;
- комбинированные;
- антисептические.
Любые мази используются после консультации со специалистом. Гомеопатические средства от насморка – самые безопасные.
Масла от насморка
Эфирные природные масла способны облегчить состояние больного при насморке.
Они обладают следующими свойствами:
- антисептическими;
- противовирусными;
- антибактериальными;
- противовоспалительными;
- иммуностимулирующими;
- общеукрепляющими.
Масла нередко входят в состав мазей и капель, но могут приниматься в качестве самостоятельной лекарственной формы (для ингаляций).
Ингаляции при насморке
Это один из самых доступных и простых способов лечения. Ингаляции можно делать с помощью эфирных масел, травяных сборов, физрастворов и пр.
- мягкое действие;
- очистка дыхательных путей;
- увлажнение слизистых;
- снятие отека;
- выведение густых выделений;
- безопасность.
- Ингаляционное лечение можно проводить при любом виде ринита у детей и взрослых.
Как правильно выбрать средство от ринита

Как избавиться от насморка? Для этого следует приобрести современное эффективное лекарство и использовать его с первых дней заболевания. Лучшее средство от насморка – это то, которое подобрано в зависимости от имеющихся симптомов и вида болезни. Кроме того, следует принимать витаминно-минеральные комплексы с целью повышения иммунитета. Социальная сеть аптек Столички предлагает возможность бронирования любого лекарства по доступным ценам.
Ринит у беременных
Оториноларинголог, хирург GMS Clinic Олег Абрамов рассказывает в своей статье о рините беременных (далее РБ).

Я не случайно выбрал эту тему после серии публикаций в социальной сети про аллергический ринит (далее АР), так как последние исследования отмечают, что хоть причина возникновения РБ до конца не ясна, сочетание АР, особенно плохо контролируемого вместе с РБ, может приводить к выраженной заложенности носа, к недостаточному поступлению кислорода, и, как следствие, к повышенной утомляемости, раздражительности, частым ОРВИ, нарушению сна, что безусловно может отразиться на развитии плода. Более того, наличие АР связано с храпом у женщин во время беременности, и вместе они могут провоцировать развитие синдрома апноэ (остановки дыхания во сне), что приводит к артериальной гипертензии, преэклампсии, замедлению внутриутробного роста плода и низким показателям по шкале Апгар. Поэтому актуальность данной проблемы только растет.
Определение и понятие
Ринит беременных — это заболевание, сопровождающееся заложенностью носа и выделениями, периодическим чиханием без признаков воспаления, аллергии, или других причин. Данное состояние может возникнуть в любой триместр беременности и обычно проходит в течение двух недель после родов.
Встречаемость
Заложенность носа — очень частая проблема во время беременности (встречается примерно в 65% случаев), которая может возникнуть из-за различных причин. РБ по разным данным встречается в 9-40% случаев, причем, в одном из последних наблюдений отмечается нарастающая встречаемость, то есть больше всего РБ наблюдается в 3 триместре — 38,9%, в том числе у тех, у кого не отмечались проблемы в 1 и 2 триместре.
Причины и механизм возникновения
Механизм возникновения до конца не изучен, и считается, что РБ возникает вследствие гормональных изменений, в частности, под влиянием прогестерона, эстрогена, ХГЧ и других гормонов, концентрация которых постепенно повышается в течение беременности. Некоторые авторы считают, что возникновение РБ связанно с ухудшением сопутствующего АР. Некоторые исследования показывают, что гормональное воздействие приводит к расслаблению гладкой мускулатуры, которая составляет стенку сосудов слизистой носа, в результате чего появляется заложенность носа. Такие выводы подтверждаются другими исследованиями, которые показывают, что оральные контрацептивы вызывают схожие эффекты в полости носа (но не у всех). Другие работы показывают, что повышенный индекс массы тела, избыточный вес, множественные беременности провоцируют или отягощают РБ.
Прогрессирование и потенциальные риски
РБ при отсутствии адекватного лечения оказывает неблагоприятное влияние на течение беременности и может приводить к развитию риносинусита, который особенно тяжело переносится в 3 триместре. С другой стороны, беременность — особый период в жизни женщины, при котором большое количество лекарств запрещены, и ЛОР патологии, эти ограничения тоже не обошли стороной. Очень часто слышу на приеме: « Доктор я беременна и мучаюсь со своим носом все это время, но врачи мне говорят — ничего не поделаешь нужно терпеть». С другой стороны, часто наблюдается обратная ситуация «Доктор, я беременная и я без сосудосуживающих капель жить не могу ». Эти ситуации, конечно же, не правильны, так как с одной стороны есть выход и оптимальное лечение, а с другой стороны постоянное воздействие сосудосуживающими препаратами — это совсем не выход из ситуации.

Диагностика
На данный момент не существует специфического теста, позволяющего подтвердить или исключить РБ. Диагноз ставится на основании жалоб пациентки и исключения других патологий полости носа.
Выбор лечебной тактики
Прежде чем рассматривать более серьезные лекарства, следует начать с наших любимых солевых растворов. Следует отметить, что речь идет не про обычные солевые растворы, а гипертонические солевые растворы (с повышенным содержанием соли, примерно 19-23 г/л). Такие спреи продаются во всех аптеках, но сразу вам их не продадут (нужно попросить). Несколько исследований отмечают достоверную эффективность в снижении заложенности при использовании их при АР, хроническом риносинусите. Также сравнительные исследования показывают их большую эффективность по сравнению с обычными изотоническими растворами. Примеры: Физиомер — гипертонический раствор (мой любимый), Аквалор-заложенность, или Аквалор-сильный насморк, Аквамарис Стронг.
Доктор, не помогает.
Как известно из прошлых публикаций, наиболее эффективным в лечении АР на сегодняшний день являются интраназальные глюкокортикостероиды (иГКС). Они обладают доказанной эффективностью в снижении заложенности носа, а так же, зуда в носу и слезотечения и позволяют добиться адекватного контроля симптомов. Но, учитывая их гормональный эффект и возможное пагубное воздействие на плод, существуют определенные риски в их применении. Так же следует отметить, что на данный момент нет исследований, предоставляющих достоверные данные, подтверждающие опасность их применения. Современные ИГКС — мометазон (назонекс, дезринит) и флутиказон (авамис, фликсоназе) обладает очень низкой системной биодоступностью, меньше 1% и доказанной эффективностью, тем самым могут рассматриваться как начальная терапия РБ. В исследованиях не было выявлено статистически значимой взаимосвязи между развитием пороков плода и применением данных средств.
Кто такие FDA в США и почему их все слушают?
Все очень просто (жаль, что у нас не все так просто). Копирую объяснение из Википедии: « Агентство Министерства здравоохранения и социальных служб США, один из федеральных исполнительных департаментов. Управление занимается контролем качества пищевых продуктов, лекарственных препаратов, косметических средств, табачных изделий и некоторых других категорий товаров, а также осуществляет контроль за соблюдением законодательства и стандартов в этой области. »
Согласно классификации FDA по влиянию лекарств на плод, будесонид (тафен назаль) относится к категории В, которая означает, что есть доказательства безопасности применения данного лекарства во время беременности. При этом биодоступность будесонида составляет 33%. Этот препарат переместился из группы С в группу В, благодаря нескольким качественно проведенным исследованиям в Швеции с начала XXI века, доказавшим его безопасность.
Так же, согласно современным рекомендациям Американской Академии Аллергологии и иммунологии (AAAAI) ИГКС считаются безопасными и эффективными средствами в лечении ринита и риносинусита во время беременности. Но при этом не отмечается указание на конкретные препараты. Другие компетентные медицинские ассоциации так же не дают какие-либо рекомендации в плане выбора препарата. Поэтому, подытоживая все выше сказанное, а также согласно данным последнего обзора мометазон, флутиказон, будесонид могут рассматриваться как безопасные и эффективные средства в терапии РБ. Также следует отметить, что назначением препарата и ведением пациента должен заниматься опытный ЛОР врач, так как эти лекарства в РФ продаются без рецепта; мы настоятельно рекомендуем не заниматься самолечением.

Да не буду я принимать эти гормоны!
В некоторых ситуациях ОРВИ во время беременности может сопровождаться (во многом благодаря сопутствующему РБ или АР или и их комбинации) затяжным насморком, заложенностью носа и тяжестью в лице — классическими симптомами риносинусита. Данное заболевание при отсутствии адекватного лечения может приводить к серьезным осложнениям, поэтому крайне важна правильная диагностика данного заболевания. Антибиотики пенициллинового ряда относятся к категории В согласно FDA и могут быть применены при лечении (ОРС). При аллергии на пеницилины также могут быть использованы некоторые цефалоспорины или линкозамиды (Клиндамицин). Все они относятся к категорям А и В. ИГКС входят в стандарты лечения острых риносинуситов (подробнее в след. публикациях) и могут обеспечить выздоровление в комбинации с солевыми растворами без антибиотиков.
P. S. Принятие решения о лечении индивидуально для каждого случая и должно быть коллективным между врачом и пациентом. Надеюсь, данный обзор позволил прояснить некоторые аспекты в особенностях РБ и дать понять, что РБ не приговор и можно его адекватно контролировать.
Физраствор – универсальное лекарство

Хлорид натрия является не просто поваренной солью, расщепленной в дистилированной жидкости, это еще и лекарство, которое называют просто физраствор.
Натрия хлорид – что это?
Лечебный солевой раствор считается отличным проводником электричества. Благодаря ему поддерживается водно-электролиный и щелочный баланс.
Получают физиологический раствор достаточно просто – пищевую соль понемногу добавляют в дистилированную воду, пока не получится необходимая концентрация. Главное вводить соль порциями, чтобы она полностью растворялась, нельзя чтобы образовывался осадок.
В некоторых случаях организму может недоставать хлорида натрия. Его дефицит может быть вызван:
большая утрата жидкости;
инфекция желудочно-кишечного тракта;
Когда используют
Раствор хлорида натрия успешно используют:
на момент операционного вмешательства и после проведения операции для поддержания объема плазмы;
при обезвоживании организма, что вызвано разными заболевания;
при сильном кровотечении, ожогах тяжелой степени и диспенсии для поддержания объема плазмы;
для уменьшения интоксикации при попадании в организм опасной инфекции;
для промывания глаз при воспалительных и инфекционных процессах, аллергиях и травмах;
для промывания носа при простудных заболеваниях;
для ингаляций при заболевании органов дыхания;
для растворения разных лекарственных препаратов при совместном использовании при инъекциях.
Способы применения
Подкожное и внутривенное введение
В медицине сейчас тяжело обойтись без использования физраствора. Он необходим при введении медикаментозных препаратов капельным способом и уколами, поскольку любое концентрированное и порошкообразное средство перед использованием нужно растворить в физиологическом растворе.
Также он позволяет сохранять объем плазмы, поддерживать водно-солевой баланс. Эффективен во время отравления, сильных отеках, для разбавления густой крови.
Раствор чаще всего вводят в организм через капельницу или подкожными инъекциями. Перед введением нужно разогреть раствор до 36-38 градусов.
При инъекциях стоит учитывать особенности организма пациента, его возраст, вес, количество утраченной жидкости и недостающего натрия и хлора.
В среднем человеку на день нужно 500 мл натрия. Именно этот объем и нужно вводить. Если утрачено очень много жидкости или отмечается сильная интоксикация, то можно увеличить до 3000 мл в сутки.
Для ребенка на 1 кг нужно 20-80 мл.
Для подкожного и внутривенного введения подходит только стерильный раствор.
Для промывания носоглотки
Физиологический раствор считается недорогим средством, которое является весьма эффективным. Хлорид натрия помогает промыть носоглотку по время простудных заболеваний. Уже после первого использования можно заметить существенное улучшение состояния, нос очищается от слизи и исчезает насморк. Промывание можно делать при аллергическом насморке, для профилактики воспалительных процессов.
Средство разрешается использовать беременным и кормящим грудью женщинам. Также его можно давать грудничкам, когда прием других медикаментов может нанести вред.
Достоинство раствора в том, что после использования слизистая поверхность носа не сушится и не травмируется. Промывать носоглотку можно несколько раз на день, нет ограничений относительно частоты использования.
Раствор можно легко приготовить самостоятельно в домашних условиях. Для этого понадобиться около 10 г поваренной соли и 1 л кипяченой воды. Раствор процедить через марлю и капать им нос. Он является нестерильным и его можно давать детям от 3х лет.
Для очищения желудка и кишечника
Раствор эффективен при сильных отравлениях. Его используют для ректальных клизм, чтобы стимулировать дефекацию. В таком случае понадобиться 3 л 9% раствора в день. перед использованием нужно разогреть раствор до 36-37 градусов, чтобы не вызывать раздражение кишечника. Подойдет нестерилизованный раствор.
Также его применяют при пищевом отравлении для промывания желудка. Раствор натрия хлорид пьют небольшими глотками, после чего нужно самостоятельно спровоцировать рвоту. Для этого необходим только стерильный раствор.
Противопоказания и побочные реакции
Хлорид натрия имеет противопоказания, с которыми стоит ознакомиться прежде чем начать лечения. Физиологический раствор нельзя принимать при:
отеках дыхательных органов;
серьезных заболеваниях сердца;
нехватке кальция в организме;
чрезмерном содержании жидкости вне клетки;
параллельном приеме кортикостероидов.
В большинстве случаев натрий хлорид хорошо переносится пациентами. Но если превышать допустимые дозы или очень долго использовать раствор, могут появиться побочные реакции:
ухудшение работы нервной системы, что проявляется тревожностью, беспокойством, слабостью, головокружением, головными болями, сильной потливостью;
сбой в работе органов пищеварения, что приводит к рвоте, тошноте, расстройству желудка;
гормональный сбой, нарушение менструального цикла;
резкое падение уровня калия в крови;
сбой в работе сердечно-сосудистой системы, учащается сердцебиение, скачет давление;
При появлении хоть одной нежелательной реакции стоит сразу же прекратить использование физиологического раствора и обратиться к врачу. Специалист оценит состояние больного, при необходимости окажет медицинскую помощь, чтобы устранить негативные эффекты.
Перед использованием также нужно проконсультироваться врачом, который сможет определить подходящую систему лечения, чтобы не допустить передозировки. По необходимости сдают анализ мочи и крови.
Все представленные на сайте материалы предназначены исключительно для образовательных целей и не предназначены для медицинских консультаций, диагностики или лечения. Администрация сайта, редакторы и авторы статей не несут ответственности за любые последствия и убытки, которые могут возникнуть при использовании материалов сайта.
Ингаляционная терапия: показания и противопоказания
Ингаляционная терапия – процедура при которой, пациент вдыхает лекарственные вещества или воздух через небулайзер. Процедура назначается как в лечебных целях, так и целях профилактики.
Цель ингаляционной терапии – доставить лекарственное вещество в определенную область дыхательных путей, при этом минимизировать накопление препарата в других органах.
Виды ингаляций
На практике применяются различные виды ингаляции, которые представлены далее:
- Паровые. Самый распространенный вид ингаляции при котором пациент вдыхает горячий пар. Процедура назначается при заболевании верхних дыхательных путей: фарингит и ринит, снимает отек.
- Тепловлажные используются с теплым воздухом и аэрозолями солей. Курс процедур способствует отхаркиванию и выведению слизи.
- Влажные разрешены тем, кому противопоказаны паровые и тепловлажные. Раствор распыляется в дыхательные пути без подогрева.
- Сухие. Воздух при таком сеансе сухой и горячий, подходит для лечения ОРЗ;
- Воздушные. Воздух распыляется с помощью баллончика, обладает бронхолитическими свойствами;
- Масляные ингаляции основаны на распылении подогретых масел, которые подходят при сухости и покрывают защитной плёнкой органы дыхания;
- Ультразвуковые ускоряют выздоровления и способствуют отхаркивания. На лекарство аппарат воздействует ультразвуком.
Разновидности аппаратов и принцип их действия
Ингаляторы разделяются на 4 вида:
1. Паровые – приборы которые нагревают вещество до газообразного состояния. При использовании данного ингалятора частицы попадают в верхние дыхательные пути.
2. Компрессорные ингаляторы. Принцип действия заключается в нагнетании воздуха под давлением при помощи компрессора.
3. Ультразвуковые – аппараты которые воздействуют ультразвуком на вещество, превращая его в аэрозоль.
4. Меш-ингаляторы. Лекарство проходит через сетку с отверстиями, создавая при этом аэрозоль.
Подобрать подходящий ингалятор поможет врач, исходя из цели процедуры.
Как проводить ингаляции
1. Прекратить приём пищи и физических нагрузок за 2 часа до сеанса;
2. Перед началом ингаляционной терапии заливается лекарство;
3. Сеанс проходит в положении сидя в расслабленном состоянии;
4. Включите ингалятор;
5. Мундштук прибора плотно обхватите губами;
6. Во время ингаляции вдыхайте полной грудью и медленно;
Длительность сеанса и лекарственные препараты назначаются исходя из диагноза лечащим врачом.
Ошибки при использовании ингалятора
Наиболее распространённые ошибки при проведении физиопроцедуры:
1. Не обрабатывать аппарат. Даже при использовании прибора одним человеком, обязательно проводить обработку ингалятора.
2. Заливать раствор в прибор, не имея представления о том, что можно применять, а что нет.
3. Проводить процедуру имея противопоказания.
4. Использовать аппарат сразу после больного.
5. Не соблюдать время проведения сеанса, назначенного врачом.
Показания к применению
- Заболевания верхних дыхательных путей (легких и бронхов);
- Бронхиальная астма;
- Заболевания среднего уха;
- Аллергический ринит;
- Профилактика простудных заболеваний;
- Остаточные явления пневмонии;
- Грипп;
- ОРВИ;
Лечебный эффект ингаляции
- Способствует выведению мокроты;
- Снимает напряжение;
- Уменьшает воспаления;
- Борется с микробами;
- Укрепляет иммунитет;
- Снимает спазм бронхов;
Противопоказания к физиопроцедуре
При всей пользе от терапии существует ряд противопоказаний, которые необходимо учитывать:
- Аллергия на применяемые растворы или его компоненты;
- Расширение альвеол легких в тяжелой форме;
- Кровотечение из носа;
- Повышенная температура тела;
- Дыхательная недостаточность;
- Заболевания сердца;
Побочное действие
При глубоком вдохе возможно головокружение и тошнота, появление кашля. Процедура безопасна, побочные эффекты могут возникнуть при наличии противопоказаний и не соблюдении рекомендаций специалиста.
Ингаляция в домашних условиях
Физиопроцедура в домашних условиях эффективно дополнит лечение простудных заболеваний, борется с кашлем и способствует выведению мокроты. Сегодня не составит труда приобрести небулайзер.
Рекомендации для ингаляции в домашних условиях:
- Не принимать пищу за 1.5 часа до сеанса;
- Если лекарство вы используете впервые, то вдыхание стоит проводить не более 2 минут, на случай выявления аллергии на препарат или активные компоненты;
- Не разговаривать в процессе ингаляции;
- После процедуры следует расслабиться и полежать 20-30 минут;
Ингаляции при помощи небулайзера безопасны и просты в применении. Процедуру в домашних условиях можно сделать с применением минеральной воды или с использованием эфирных масел.
Минеральная вода способствует выведению и разжижению мокроты.
Эфирные масла смягчают слизистую и облегчают дыхание.
Ингаляция для детей
Ингаляцию для ребёнка можно проводить с 2 лет, но только по рекомендации врача. Паровые ингаляции запрещены.
1. Проводите процедуру каждый день в одно и тоже время, чтобы ребёнок привык.
2. Отвлеките ребёнка: читать книжку, дать игрушку или включить любимые мультики.
3. Если ребёнок вел себя спокойно и соблюдал все правила, похвалите его в конце.
Что заливать в ингалятор
В зависимости от того, какую цель преследует ингаляция препарат подбирается индивидуально. Вдыхание веществ намного эффективнее чем прием таблеток, так как активные компоненты действую локально. Однако не стоит пренебрегать лечением. В небулайзер заливают такие растворы как: эфирные масла, физрастворы и лекарства.
Лекарства для небулайзера
Препарат и его дозировка назначаются только лечащим врачом, не стоит заниматься самолечением. Существует 5 групп, которые используются при физиопроцедуре.
- Бронхолитики используют для лечения бронхиальной астмы и хронического заболевания лёгких.
- Нестероидные противовоспалительные препараты — снимают болевые ощущения и воспаления, применяются при лихорадке.
- Антибиотики назначают при бактериальных инфекциях.
- Кортикостероиды — стероидные средства, которые эффективны в борьбе с воспалительными процессами.
- Муколитики — разжижают мокроту и способствуют выведению слизи из лёгких.
Эфирные масла
Жидкость, которую можно заливать только в паровые ингаляторы. Масла доказывают свою эффективность при профилактике гриппа и ОРВИ. Чаще остальных применяют масла эвкалипта, чайного дерева и аниса.
Физраствор
Физраствор – жидкость, которая состоит из воды и натрий хлора 0,9%. Данное соединение безопасно и подходит даже для ребёнка. Аналог раствора можно сделать в домашних условиях из дистиллированной воды и поваренной соли. Состав ускоряет выведение мокроты и смягчает слизистую. Минеральная вода боржоми считается аналогом физраствора.
Заключение
Ингаляционная терапия пользуется популярностью среди физиопроцедур и решает ряд проблем, выступает в целях профилактики и лечения заболеваний дыхательных путей. Процедура безопасна для пациентов любых возрастов. Вдыхание лекарственных веществ при помощи пара приобретает особую значимость при лечении органов дыхания.

Для людей, страдающих респираторными заболеваниями, ингалятор — незаменимый помощник. Чтобы ингалятор выполнял свою функцию и пациенты получали полноценное лечение, необходимо понимание как правильно использовать ингалятор. Однако более 50% пациентов не знают как правильно дышать ингалятором, поэтому их болезни не получают необходимого лечения, в результате чего могут негативно повлиять на здоровье.
Разберем на примере одного из очень распространенных респираторных заболеваний, когда люди принимают лекарства, вводимые через ингалятор, — астма.
Астма это хроническое воспалительное заболевание дыхательных путей, проявляющееся одышкой, хрипом, тяжестью в груди и кашлем. При лечении астмы врачи назначают так называемое поддерживающее лечение, при котором пациент регулярно вдыхает лекарство с помощью ингаляционной системы (ингалятора).
Это может показаться простым, но люди все равно совершают ошибки, которые затем существенно влияют на курс лечения.
Как правильно дышать ингалятором?
Вот четыре универсальных ошибки, которые возникают при использовании любого типа ингалятора:
1. Не дышать перед вдохом
Первая ошибка, которую часто совершают люди, — это не сделать глубокий выдох перед использованием ингалятора. Перед каждым использованием ингалятора всегда максимально полностью выдыхайте за пределы ингалятора.
Это создаст в легких больше места для следующего глубокого вдыхания активного вещества из ингалятора. Таким образом, вдыхаемый препарат лучше проникает в дыхательные пути и будет наиболее эффективным.
2. Задерживайте дыхание на рекомендованное время.
Также важно не забывать задерживать дыхание хотя бы на 5 секунд сразу после глубокого вдыхания лекарства путем ингаляции. В это время дыхательные пути находятся в состоянии покоя, что дает лекарству больше времени, чтобы осесть в легких и начать действовать.
Идеально, задержать дыхание в течение 5-10 секунд, но если это невозможно, постарайтесь продержаться так долго, на сколько это возможно.
3. Выдох в систему ингалятора.
Еще одна распространенная ошибка — выдохнуть обратно в ингалятор. Поэтому, задержав дыхание как минимум на 5 секунд, чтобы вещество могло попасть в легкие, выньте ингалятор изо рта и выдохните наружу.
4. Не прикладывать ингалятор к губам.
Последняя ошибка, которую совершают люди, — не прикладывают к губам ингалятор. Поэтому перед использованием ингалятора всегда следите за тем, чтобы ваши губы плотно прилегали к мундштуку ингалятора, чтобы доза не попала в ту область, где она теряет свои свойства.
Ингалятор для лечения респираторных и других заболеваний вы можете приобрести с доставкой в нашем интернет магазине или в одном из наших магазинов по адресу:
ул. Оборонная 8
ТЦ Горизонт 1 этаж,ул. Большая, 88
ТЦ Южный парк 1 этаж бутик 131, ул.Суворова,25
По всем вопросам звоните 8-924-309-39-84 или 900-505, будем рады помочь.
Ингаляционная терапия – процедура при которой, пациент вдыхает лекарственные вещества или воздух через небулайзер. Процедура назначается как в лечебных целях, так и целях профилактики.
Цель ингаляционной терапии – доставить лекарственное вещество в определенную область дыхательных путей, при этом минимизировать накопление препарата в других органах.
Виды ингаляций
На практике применяются различные виды ингаляции, которые представлены далее:
- Паровые. Самый распространенный вид ингаляции при котором пациент вдыхает горячий пар. Процедура назначается при заболевании верхних дыхательных путей: фарингит и ринит, снимает отек.
- Тепловлажные используются с теплым воздухом и аэрозолями солей. Курс процедур способствует отхаркиванию и выведению слизи.
- Влажные разрешены тем, кому противопоказаны паровые и тепловлажные. Раствор распыляется в дыхательные пути без подогрева.
- Сухие. Воздух при таком сеансе сухой и горячий, подходит для лечения ОРЗ;
- Воздушные. Воздух распыляется с помощью баллончика, обладает бронхолитическими свойствами;
- Масляные ингаляции основаны на распылении подогретых масел, которые подходят при сухости и покрывают защитной плёнкой органы дыхания;
- Ультразвуковые ускоряют выздоровления и способствуют отхаркивания. На лекарство аппарат воздействует ультразвуком.
Разновидности аппаратов и принцип их действия
Ингаляторы разделяются на 4 вида:
1. Паровые – приборы которые нагревают вещество до газообразного состояния. При использовании данного ингалятора частицы попадают в верхние дыхательные пути.
2. Компрессорные ингаляторы. Принцип действия заключается в нагнетании воздуха под давлением при помощи компрессора.
3. Ультразвуковые – аппараты которые воздействуют ультразвуком на вещество, превращая его в аэрозоль.
4. Меш-ингаляторы. Лекарство проходит через сетку с отверстиями, создавая при этом аэрозоль.
Подобрать подходящий ингалятор поможет врач, исходя из цели процедуры.
Как проводить ингаляции
1. Прекратить приём пищи и физических нагрузок за 2 часа до сеанса;
2. Перед началом ингаляционной терапии заливается лекарство;
3. Сеанс проходит в положении сидя в расслабленном состоянии;
4. Включите ингалятор;
5. Мундштук прибора плотно обхватите губами;
6. Во время ингаляции вдыхайте полной грудью и медленно;
Длительность сеанса и лекарственные препараты назначаются исходя из диагноза лечащим врачом.
Ошибки при использовании ингалятора
Наиболее распространённые ошибки при проведении физиопроцедуры:
1. Не обрабатывать аппарат. Даже при использовании прибора одним человеком, обязательно проводить обработку ингалятора.
2. Заливать раствор в прибор, не имея представления о том, что можно применять, а что нет.
3. Проводить процедуру имея противопоказания.
4. Использовать аппарат сразу после больного.
5. Не соблюдать время проведения сеанса, назначенного врачом.
Показания к применению
- Заболевания верхних дыхательных путей (легких и бронхов);
- Бронхиальная астма;
- Заболевания среднего уха;
- Аллергический ринит;
- Профилактика простудных заболеваний;
- Остаточные явления пневмонии;
- Грипп;
- ОРВИ;
Лечебный эффект ингаляции
- Способствует выведению мокроты;
- Снимает напряжение;
- Уменьшает воспаления;
- Борется с микробами;
- Укрепляет иммунитет;
- Снимает спазм бронхов;
Противопоказания к физиопроцедуре
При всей пользе от терапии существует ряд противопоказаний, которые необходимо учитывать:
- Аллергия на применяемые растворы или его компоненты;
- Расширение альвеол легких в тяжелой форме;
- Кровотечение из носа;
- Повышенная температура тела;
- Дыхательная недостаточность;
- Заболевания сердца;
Побочное действие
При глубоком вдохе возможно головокружение и тошнота, появление кашля. Процедура безопасна, побочные эффекты могут возникнуть при наличии противопоказаний и не соблюдении рекомендаций специалиста.
Ингаляция в домашних условиях
Физиопроцедура в домашних условиях эффективно дополнит лечение простудных заболеваний, борется с кашлем и способствует выведению мокроты. Сегодня не составит труда приобрести небулайзер.
Рекомендации для ингаляции в домашних условиях:
- Не принимать пищу за 1.5 часа до сеанса;
- Если лекарство вы используете впервые, то вдыхание стоит проводить не более 2 минут, на случай выявления аллергии на препарат или активные компоненты;
- Не разговаривать в процессе ингаляции;
- После процедуры следует расслабиться и полежать 20-30 минут;
Ингаляции при помощи небулайзера безопасны и просты в применении. Процедуру в домашних условиях можно сделать с применением минеральной воды или с использованием эфирных масел.
Минеральная вода способствует выведению и разжижению мокроты.
Эфирные масла смягчают слизистую и облегчают дыхание.

Ингаляция для детей
Ингаляцию для ребёнка можно проводить с 2 лет, но только по рекомендации врача. Паровые ингаляции запрещены.
1. Проводите процедуру каждый день в одно и тоже время, чтобы ребёнок привык.
2. Отвлеките ребёнка: читать книжку, дать игрушку или включить любимые мультики.
3. Если ребёнок вел себя спокойно и соблюдал все правила, похвалите его в конце.
Что заливать в ингалятор
В зависимости от того, какую цель преследует ингаляция препарат подбирается индивидуально. Вдыхание веществ намного эффективнее чем прием таблеток, так как активные компоненты действую локально. Однако не стоит пренебрегать лечением. В небулайзер заливают такие растворы как: эфирные масла, физрастворы и лекарства.
Лекарства для небулайзера
Препарат и его дозировка назначаются только лечащим врачом, не стоит заниматься самолечением. Существует 5 групп, которые используются при физиопроцедуре.
- Бронхолитики используют для лечения бронхиальной астмы и хронического заболевания лёгких.
- Нестероидные противовоспалительные препараты — снимают болевые ощущения и воспаления, применяются при лихорадке.
- Антибиотики назначают при бактериальных инфекциях.
- Кортикостероиды — стероидные средства, которые эффективны в борьбе с воспалительными процессами.
- Муколитики — разжижают мокроту и способствуют выведению слизи из лёгких.
Эфирные масла
Жидкость, которую можно заливать только в паровые ингаляторы. Масла доказывают свою эффективность при профилактике гриппа и ОРВИ. Чаще остальных применяют масла эвкалипта, чайного дерева и аниса.
Физраствор
Физраствор – жидкость, которая состоит из воды и натрий хлора 0,9%. Данное соединение безопасно и подходит даже для ребёнка. Аналог раствора можно сделать в домашних условиях из дистиллированной воды и поваренной соли. Состав ускоряет выведение мокроты и смягчает слизистую. Минеральная вода боржоми считается аналогом физраствора.
Заключение
Ингаляционная терапия пользуется популярностью среди физиопроцедур и решает ряд проблем, выступает в целях профилактики и лечения заболеваний дыхательных путей. Процедура безопасна для пациентов любых возрастов. Вдыхание лекарственных веществ при помощи пара приобретает особую значимость при лечении органов дыхания.

Читайте в этой статье:
-
Что такое ингаляция?
-
Самостоятельный выбор лекарств
-
Использование лекарств на основе масел
-
Неправильная продолжительность и частота ингаляций
-
Использование небулайзера после другого человека
-
Отмена ингаляций при повышении температуры
-
Неправильное дыхание
-
Проведение ингаляций при любой простуде
-
Использование мундштука для детей младше 5 лет
-
Эффективные ингаляции по всем правилам
Небулайзеры – это устройства, распыляющие лекарственные вещества в виде аэрозоля. При вдыхании мельчайшие частички препаратов попадают в дыхательные пути и воздействуют непосредственно на очаг заболевания. Приборы дают возможность точно дозировать раствор и предотвращают побочные эффекты, которые возникают при лечении сиропами или таблетками. Но несоблюдение правил при ингаляции может существенно снизить эффективность лечения, а иногда и нанести вред организму.
Что такое ингаляция?
Чтобы правильно выполнять процедуру, стоит разобраться, что такое ингаляция, каковы ее цели и особенности. Под этим термином понимается вдыхание лекарственных веществ в аэрозольной форме. Процедура проводится с помощью специальных приборов – ингаляторов или небулайзеров, которые превращают раствор для ингаляции в мельчайшие частички.
Попадание этих частиц на слизистую оболочку системы дыхания оказывает комплексное воздействие: блокирует воспаление, снимает отек, способствует выводу слизи и мокроты, оказывает увлажняющее действие. Все это помогает сократить симптомы, ускоряет процесс лечения, улучшает самочувствие.
Ингаляторы могут использоваться в амбулаторных и домашних условиях. Их применяют для взрослых и для детей любого возраста при отсутствии противопоказаний. Ингаляции эффективны при респираторных вирусных инфекциях и бронхитах, при астме и пневмонии, некоторых других заболеваниях. Такая процедура служит хорошей профилактикой болезней ЛОР-органов и помогает справиться с осложнениями после коронавирусной инфекции.

Но все эти положительные свойства проявляются только при правильном использовании приборов, поэтому стоит знать о наиболее частых ошибках, которые допускаются при использовании небулайзеров.
Самостоятельный выбор лекарств
Одной из наиболее частых и при этом самых опасных ошибок являются попытки самолечения. Важно помнить, что лекарство для ингаляционной терапии должен назначать врач с учетом клинической картины, сопутствующих заболеваний, возраста и прочих нюансов.
Например, известно, что ингаляции помогают при кашле. Но если человек покупает в аптеке отхаркивающее средство на свое усмотрение, вполне могут проявиться бронхообструкции. Не исключено увеличение объема мокроты. Врач при подборе препарата определяют тип кашля, степень вязкости мокроты, сужаемость просветов в бронхах, наличие бронхоспазма и отека слизистой. Только на основании всех этих факторов доктор подбирает подходящий лекарственный раствор.
Использование лекарств на основе масел
Масляный раствор содержит жиры, которые оседают на легких во время ингаляции. Это приводит к нарушению газообмена и может стать причиной опасных осложнений. Существует даже такой термин – масляная пневмония. К тому же составы, содержащие масло, нарушают работу небулайзера, выводят его из строя, и восстановить работоспособность устройства зачастую уже невозможно.

Неправильная продолжительность и частота ингаляций
Время ингаляции в каждом случае определяется врачом в зависимости от вида заболевания, его сложности, характеристик применяемого лекарства и прочих факторов. В среднем процедура проводится трижды в день, через час после еды. За это время повышается внутрибрюшное давление, за счет воздействия внутренних органов на диафрагму сокращается дыхательный объем.
Если ингаляции назначены для разжижения мокроты, делать их нужно не меньше, чем за 4 часа до сна, чтобы успеть откашляться. В ином случае сон будет нарушен постоянным кашлем, который усилится при горизонтальном положении тела либо мокрота будет застаиваться, а утром начнутся приступы продуктивного кашля. При использовании бронходилаторов ингаляции проводятся за час до сна, это связано со стимулированием сердца и сосудов. В любом случае, необходимо четко следовать рекомендациям врача относительно времени ингаляций.
Использование небулайзера после другого человека
Обычно в семье имеется один небулайзер, и если заболевает сразу несколько домочадцев, все они пользуются одним прибором. Ключевое правило в этом случае – обязательная обработка съемных элементов ингалятора после каждой процедуры. Подробная информация об очистке прибора есть в инструкции. Только при таком подходе можно избежать перекрестных инфекций и проводить процедуры всем членам семьи.
Отмена ингаляций при повышении температуры
Многие считают, что при повышенной температуре (гипертермии) ингаляции делать нельзя. На самом деле это не совсем так. Подобные состояния служат противопоказанием только для проведения процедуры с помощью парового ингалятора. Небулайзеры других типов могут использоваться и при повышенной температуре, если врач не дал других указаний. Однако при ухудшении самочувствия во время процедуры необходимо сразу ее прекратить.
Неправильное дыхание
Во время ингаляции нужно дышать ровно и спокойно. Если прибор используется для лечения заболеваний трахеи, гортани или глотки, нужно делать вдох через рот, на 2 секунды задерживать дыхание, после чего делать полный выдох через нос. При лечении болезней носоглотки, околоносовых пазух и носа вдох и выдох делаются через нос. Во втором случае используются специальные канюли или маска.

Важно помнить, что глубокое дыхание во время ингаляции вызывает гипервентиляцию легких, из-за чего возникает головокружение.
Проведение ингаляций при любой простуде
Ингаляция – это эффективный метод лечения бронхитов, пневмоний, трахеитов, снятия симптомов бронхиальной астмы. В этом случае целесообразна доставка частиц действующего вещества глубоко в органы дыхания, где они оседают в высокой концентрации. А вот лечение фарингита или насморка таким способом не даст ожидаемого эффекта, поскольку на слизистой носа и глотки задержится совсем немного частиц.
Использование мундштука для детей младше 5 лет
Ребенок в таком возрасте не всегда может дышать правильно, делая вдох ртом через мундштук. Маска помогает добиться оптимальной концентрации лекарственного вещества и упростить процедуру в целом. Но она должна плотно прилегать к лицу, иначе эффективность ингаляции снизится.
Эффективные ингаляции по всем правилам
Перед использованием небулайзера необходимо проконсультироваться с врачом, а затем соблюдать все его рекомендации при проведении ингаляций. Стоит знать и об основных ошибках, которые снижают эффективность процедуры, чтобы не допускать их во время лечения.
- Review
- Open Access
- Published: 16 January 2018
- Federico Lavorini2,
- Jonathan Marshall3,
- William Christopher Nigel Dunlop3,
- Louise Heron4,
- Emily Farrington4 &
- …
- Richard Dekhuijzen5
Respiratory Research
volume 19, Article number: 10 (2018)
Cite this article
-
22k Accesses
-
153 Citations
-
129 Altmetric
-
Metrics details
Abstract
Background
Inhaled drug delivery is the cornerstone treatment for asthma and chronic obstructive pulmonary disease (COPD). However, use of inhaler devices can be challenging, potentially leading to critical errors in handling that can significantly reduce drug delivery to the lungs and effectiveness of treatment.
Methods
A systematic review was conducted to define ‘critical’ errors and their impact on health outcomes and resource use between 2004 and 2016, using key search terms for inhaler errors in asthma and COPD (Search-1) and associated health-economic and patient burden (Search-2).
Results
Search-1 identified 62 manuscripts, 47 abstracts, and 5 conference proceedings (n = 114 total). Search-2 identified 9 studies. We observed 299 descriptions of critical error. Age, education status, previous inhaler instruction, comorbidities and socioeconomic status were associated with worse handling error frequency. A significant association was found between inhaler errors and poor disease outcomes (exacerbations), and greater health-economic burden.
Conclusions
We have shown wide variations in how critical errors are defined, and the evidence shows an important association between inhaler errors and worsened health outcomes. Given the negative impact diminished disease outcomes impose on resource use, our findings highlight the importance of achieving optimal inhaler technique, and a need for a consensus on defining critical and non-critical errors.
Background
Inhaled drug delivery is the cornerstone of therapy for the treatment of obstructive chronic airway diseases, such as asthma and chronic obstructive pulmonary disease (COPD) [1]. The most common devices used to administer aerosolized medication in day-to-day respiratory practice are the pressurized metered-dose inhaler (pMDI) and the dry powder inhaler (DPI). pMDIs are most often prescribed [2], but patients need to inhale correctly and coordinate breathing and actuation to ensure effective drug delivery [3,4,5,6]. In contrast, DPIs are breath-actuated, with most devices relying on a rapid and powerful inhalation manoeuvre for drug delivery, which can be particularly problematic for patients who struggle to inhale forcefully [6].
Recent advances in inhaler technologies have seen an explosion in the number of devices [7]. This plethora of devices, however, has led to confusion in their use amongst health-care providers (HCPs) and patients, who may not properly understand how to use inhalers [8]. Indeed, mastering an inhaler device involves correct preparation and handling of the device before inhalation, and an optimal inhalation technique; an error in any step of this process may lead to inadequate drug delivery to the lungs.
There is no one ‘perfect device’ and several studies have shown that inhaler technique errors made by patients with asthma and COPD are common in real life with both pMDIs and DPIs despite advances in inhaler device technology [3, 9,10,11,12]. Although study results vary, estimates of those making inhaler errors range up to 90% of patients irrespective of the device type used [13, 14]. Most importantly, it is vital to distinguish between ‘critical’ (sometimes defined as ‘essential’ or ‘crucial’) errors, which are likely to significantly impair the delivery of adequate medication to the lungs, and ‘non-critical’ errors, which are likely to result in a reduced amount of drug reaching the lungs compared with that attained using the correct technique [15, 16].
A recent major cross-sectional study of asthma patients has compared inhaler technique data with data on disease control, in order to determine which errors are most associated with poor health outcomes [17]. The results of this may provide the most coherent basis for defining and identifying critical errors; however, progress towards fully elucidating these errors is slow.
The societal and health-economic burden of poor inhaler technique is increasingly being recognised [10]. Worryingly, in three countries (the UK, Spain and Sweden) poor inhaler technique accounted for over €750 million in direct and indirect costs in 2015, for the two most commonly used DPIs [18]. These cost data, together with the increasing prevalence of obstructive lung diseases and restriction in healthcare spending is propagating the imperative need for inhaler competency (that is, correct and effective inhaler use) [15].
Recent global position documents from the Global Initiative for Asthma (GINA) and Global Initiative for Chronic Obstructive Lung Disease (GOLD) both give significant prominence to assessing and correcting poor inhalation technique before escalating drug therapy [19, 20].
Price et al. proposed the need for policy change and research focusing on current gaps in knowledge: specifically on the association between device errors and health economic and clinical outcomes, and on the patient characteristics associated with a higher frequency of errors [15]. Indeed, clinicians must recognise that the device itself and its characteristics are at least equally as important as the prescribed drug; and that in future, the choice of drug compound may be considered to be of secondary importance [3].
The aim of this study was to define ‘critical’ errors and their impact on health outcomes and resource use between 2004 and 2016. This was accomplished through systematically reviewing the scientific literature on inhaler errors made by patients when using pMDIs and DPIs, and the approaches used to assess them — exploring the relationships between inhaler errors, disease outcomes, quality of life, and healthcare resource use, and associations between patient characteristics and inhaler errors. Given the striking variety of inhaler errors reported in the literature [11], this paper focuses on critical errors, as these are most likely to have a health impact.
Methods
Overview
This systematic review was undertaken in accordance with the methodological and reporting standards recommended by PRISMA [21], and was registered in the PROSPERO international prospective register of systematic reviews (CRD42016036118). The review consisted of two distinct searches: search-1 focused on definitions and descriptions of critical errors, and search-2 aimed to identify the literature regarding economic models on the cost of critical errors and patient burden (see Additional file 1: Table S1).
Inclusion criteria
Studies from search-1 were included if they reported data on inhaler errors with pMDI and/or DPIs in patients with asthma or COPD, and if they related inhaler technique to disease outcomes or quality of life (QoL). Studies from search-2 were included if they reported data on the patient and/or economic burden of inhaler errors. Soft-mist inhalers and nebulisers were not considered in either search, as pMDIs and DPIs are estimated to make up around 99.8% of the global market share of inhaler devices [22].
Both searches were conducted, reviewed, and each article checked, by two authors (LH, EF) in four online databases (Embase, Medline, EconLIT and Evidence-Based Medicine Reviews), limited to studies published in English between 2004 and May 2016. International conference proceedings from 2013 to 2016 were also scanned (see Additional file 1: Table S1). All the authors reviewed the finalized list of selected articles for approval.
Data extraction
The following data were recorded from each selected article: author and contact details; number of patients; patient characteristics including age, gender, education, comorbidities, socioeconomic class, concurrent device use, and previous instruction; type(s) of inhaler; type(s) of inhaler error(s); definition of critical error(s); type of disease (asthma, COPD, or both); and findings on disease outcomes or QoL.
We grouped the emergent themes into 5 domains in our systematic review; (1) patient characteristics, (2) educational aspects, (3) disease outcomes, (4) quality of life, (5) health economics. This qualitative assessment of the study results allowed results to be reported more clearly, in order to help explore the impact of critical errors on health outcomes and resource use.
When studies were examined for evidence of an association between patient characteristics and presence or rate of inhaler errors, an a priori predefined list of characteristics agreed by consensus between the authors was used to focus analysis. This included: patient age, gender, socioeconomic class, education level, inhaler education, comorbidities, and the number of inhaler devices prescribed at the same time.
Additionally, the reference lists of all retrieved papers were reviewed for any potentially relevant studies, and editorials, commentaries, case studies, letters and opinion pieces were excluded. Studies examining nebuliser inhaler errors or those pooling nebulizer inhaler errors data with data for other inhalers were excluded, as our aim was to assess inhaler devices that administer a single discrete dose. Studies that did not specify inhaler types were included, as it was considered likely that pMDIs and DPIs would have been used, due to these of inhaler types comprising the majority of market share [23]. Descriptive methods were used to analyse data for the associations mentioned above.
Results
Search results
Initially (not including grey literature), Search-1 yielded 114 studies: 62 of these were full-text articles and 52 were abstracts. Of these, five abstracts were identified as having an economics focus and were therefore moved to the results of Search-2 (Fig. 1). Following the addition of five grey literature abstracts, the total yield of Search-1 was again 114 studies.
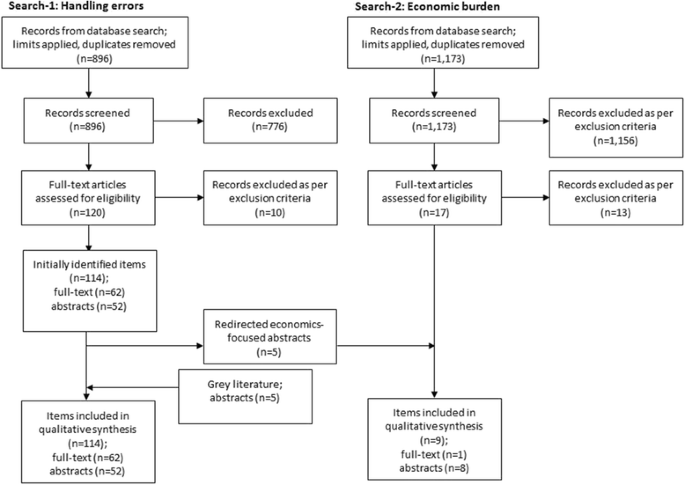
PRISMA diagram. The database search and analysis in Search-1 initially yielded 114 full-text articles or abstracts; give abstracts were removed and incorporated into the results of Search-2 due to being economics-focused; a further five abstracts were added to Search-1 following the grey literature search. Therefore, the final yield of Search-1 was 114
Full size image
All studies (n = 114) in Search-1 reported inhaler error data on pMDIs with or without spacers, and single- or multiple-dose DPIs (Fig. 2a and b). Study details including population age, respiratory disease, and inhaler device type are presented in Table 1.
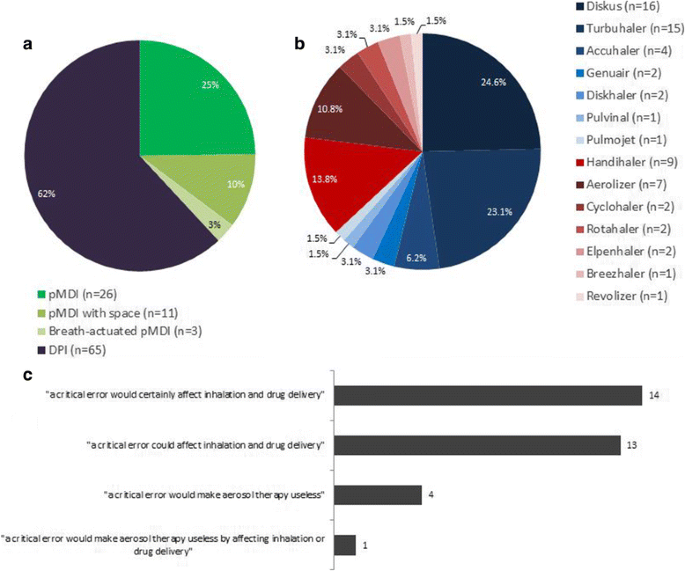
a. Journal articles reporting critical inhaler errors for pMDIs and DPIs. Note: percentages are calculated as a proportion of total mentions (n = 105) of each inhaler type by all inhaler error studies. Individual studies may mention more than one inhaler type. b. Journal articles reporting critical inhaler errors for specific DPI device types, both multi-dose (blue) and single-dose (red). Note: percentages are calculated as a proportion of total mentions (n = 65) of all device types by all inhaler error studies. Individual studies may mention more than one inhaler type. c. Studies stating a definition of a critical error, separated into categories. Details of each study and the exact wording used by each are presented in Additional file 1: Table S4. Note: In this figure the term “critical error” refers to both critical errors and critical steps that, when performed incorrectly, constitute critical errors
Full size image
Full size table
Search-2 on the health-economic burden of inhaler errors yielded only one full-text article and three abstracts that fulfilled the inclusion criteria, to which five abstracts from Search-1 were added (Fig. 1).
Definition of critical inhaler errors
Among the 36 studies giving specific examples of ‘critical’ errors, 32 included a definition of ‘critical’ inhaler errors, and the definition itself substantially varied between the studies (Fig. 2c). In most cases, studies did not provide information on the origin of their definition of a critical error; however, where this information was provided, definitions were commonly taken from previous studies, rather than being formulated by the study researchers. Astonishingly, our search yielded 299 descriptions of critical errors across the device types.
The most common definition was an action affecting the lung deposition of inhaled drug, resulting in little or no medicine being inhaled or reaching the lungs (n = 27), where 14 definitions stated a critical error “would” certainly affect inhalation and drug delivery [24,25,26,27,28,29,30,31,32,33,34,35,36,37], and 13 others said a critical error “could” affect these [38,39,40,41,42,43,44,45,46,47,48,49,50]. Conversely, 4 papers defined a critical error in terms of effectiveness: that is, an error that would make aerosol therapy useless [10, 51,52,53]; and Pascual used a combined definition of deposition and effectiveness: that is, “an error that compromised the potential benefit of the treatment, such as impeding drug deposition or the delivery of an insufficient dose” [54].
Surprisingly, only sixty studies (53%) used a checklist to quantify errors and to enable comparisons between devices. However, these checklists were often created by the authors themselves (either taken from previous studies, or were copied from the instructions provided with the inhaler device), without external validation of the checklist itself for each device type. The number of critical errors described varied by device type and by study (Additional file 1: Table S2).
To further compound matters, there were also differences in the descriptions of the actual errors themselves. For example, one DPI error was described in four different ways: two studies mentioned the critical steps which, if not performed, would be errors: “slide lever as far as possible” [42]; “push lever back completely” [27]; and two gave differing terminology for the critical error: “failure to slide the lever until the ‘click’ sound” [51] and “not sliding back the lever until a click is heard” [30]. Similarly, there were also differences in agreement between the authors of the different studies in the categorization of a critical error versus a non-critical error, once again affecting attempts to compare studies and collectively understand the impact of inhaler errors in daily clinical practice. For example, not holding the inhaler upright whilst using a pMDI was referred to as a critical error or step by three studies [39, 42, 44], but Bryant defined it simply as an “error” [55].
While many studies reported associations between characteristics or patient experiences and errors, these did not specify whether associations existed with critical errors specifically, or with all errors.
Effects of patient characteristics on frequency of inhaler errors
Overall, 41 studies of 114 (36%) investigated the effect of predefined patient characteristics on inhaler error frequency (Table 1), with patient age, gender, level of education, number of devices prescribed, and previous inhaler instruction being the most commonly explored factors.
Of 33 studies which examined the effect of patient age [10, 26, 30, 33, 34, 38, 40, 44, 48, 53, 55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77], 29 were in adults and 4 were paediatric. Only twelve studies (36%) reported age to be significantly associated with worsening frequency of inhaler errors [10, 26, 30, 44, 53, 57, 60, 64, 66, 69, 72, 73], whereas 21 studies found no significant association. In 7 studies, older adults were found to make significantly more errors [10, 30, 44, 57, 60, 64, 66]. Of the 4 paediatric studies [26, 40, 53, 74], two reported a significant association between age and frequency of errors: Deerojanawong reported that younger children made errors significantly more frequently [26], while Capanoglu reported the opposite finding: that older children made errors more frequently [53]. Twenty-five studies of 114 (22%) reported on the effects of gender [10, 30, 34, 38, 40, 44, 48, 53, 55, 56, 59,60,61, 63, 65,66,67, 70, 73, 74, 76,77,78,79,80], where 6 studies concluded a significant impact on inhaler error frequency, but the results were contradictory and inconclusive as to whether male or female gender was associated with poor technique [48, 53, 60, 66, 79, 80]. Of the 22 studies that reported a trend between low education and high inhaler error frequency [10, 34, 38, 44, 48, 53, 56, 59,60,61,62, 64,65,66,67, 70, 73,74,75,76, 80, 81], 10 found the association to be statistically significant [10, 34, 48, 53, 56, 60, 62, 66, 73, 80].
Of the 114 articles, 21 studies (18%) explored the relationship between previous inhaler instruction and inhaler error frequency [10, 25, 26, 30, 36, 39, 40, 44, 48, 53, 61, 62, 66,67,68, 71, 72, 74, 76, 80, 81], where 11 studies found previous education or instruction to be significantly related to better inhaler technique [10, 36, 39, 44, 48, 53, 61, 66, 68, 76, 80]. One study by Al-Jahdali reported a significant relationship between ‘lack of education about medication’ and improper device use [67], and two reported that reduced error frequency among previously instructed patients was dependent on device type, where technique improved only in patients using MDI spacer [26] or Diskus or Turbuhaler. [30] Interestingly, a third of studies (n = 7) reported that previous instruction in inhaler use did not significantly affect inhaler technique [25, 40, 62, 71, 72, 74, 81].
Specifically, we noted a statistically significant relationship was reported between increased error frequency and other patient characteristics such as having the presence of two or more comorbidities [56], obesity [48], heart disease [80], cognitive impairment or neuropathy [79], and lower socioeconomic class [56]. There were contradictory results between three studies that reported significant results for whether a higher or lower number of devices prescribed concurrently impacts error frequency [25, 44, 82].
Effects of educational intervention on frequency of inhaler errors
Educational interventions and their relationship to inhaler errors were addressed in 52 articles [27,28,29, 34, 37, 39, 45, 49,50,51, 54, 57,58,59, 61, 83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119], but studies varied in how errors were assessed (the tools used), by whom (the healthcare personnel), and in the duration of intervention. Interventions were undertaken by face-to-face consultation with a variety of HCPs involving physicians (n = 5), nurses (n = 5), paramedics (n = 1), and pharmacists (n = 8). In other studies, a video (n = 5), leaflet instructions (n = 17), or an online program were used (n = 2). Thirty-two studies undertook patient assessments before and after the educational intervention [29, 34, 39, 45, 51, 57,58,59, 61, 83,84,85,86,87,88,89,90,91,92, 94, 95, 97, 100,101,102,103,104, 108, 109, 114, 115]. Where 26 studies positively reported a significant improvement in inhaler technique following the intervention [29, 34, 39, 51, 57, 58, 61, 83,84,85,86,87,88,89, 92, 94, 95, 97, 101, 103, 104, 108, 109, 114, 115].
Analysis of interventions noted that the majority of the pharmacist-led studies, seven of the eight, demonstrated a statistically significant improvement in inhaler technique [39, 61, 84, 87, 91, 101, 103]. Of the five nurse-led interventions [34, 58, 85, 90, 99], three succeeded in significantly improving inhaler technique [34, 58, 85], and two reported a decrease in inhaler error frequency but did not include a statistical analysis [90, 99]. A further six HCP studies reported statistically significant improvements: three physician-led interventions, a physician-and therapist-led study, GP assistant study and a paramedic-led study all reported statistically significant improvements [57, 83, 89, 92, 94, 97]. Four studies with unspecified instructor types reported improvement [45, 51, 95, 102], but only two provided statistical analysis [51, 95]. Of the leaflet-based intervention studies (n = 17) [27,28,29, 37, 45, 49, 50, 54, 88, 93, 104, 106, 107, 112, 115, 118, 119], five compared inhaler technique before and after the intervention, of which four reported a significant improvement in inhaler technique [29, 88, 104, 115].
Association between disease outcomes and inhaler errors
Thirty-six of the 114 studies (Table 1) examined disease outcomes in relation to inhaler errors or inhalation technique (see Table 2 for a summary of available odds ratios). In the assessment of asthma control, the most common measurements were the Asthma Control Questionnaire (ACQ) and Asthma Control Test (ACT) instruments. [120, 121] Other measurements included: the Control of Allergic Rhinitis and Asthma Test [122], Asthma Therapy Assessment Questionnaire [123], Test For Respiratory And Asthma Control In Kids scales [124], frequency of exacerbations, emergency healthcare use, or general classification of patients into levels of disease control using the Global Initiative for Asthma (GINA) criteria. For COPD patients, disease outcomes were measured by: Baseline Dyspnoea Index (BDI), rates of exacerbations, hospitalizations, or by degree of dyspnoea using the modified Medical Research Council (MRC) questionnaire.
Full size table
Our systematic analysis revealed 10 studies observed a higher inhaler error frequency was significantly associated with poor disease outcomes, primarily in asthma (n = 9), but also in asthma and COPD (n = 1) [10, 38, 48, 53, 56, 57, 67, 78, 90, 97, 117]. Molimard reported that using a device incorrectly, irrespective of the type, was associated with an increased Asthma Control Score [42], and in another study by Kuprys-Lipinska and Wiacek, over 94% of patients reported an association between improved DPI technique and better disease outcomes in asthma and COPD; however, no statistical analysis was provided [100, 109]. Groot reported that incorrect inhaler technique with unspecified inhalers was the underlying cause of poor asthma control in 7.8% of its population, but again did not provide statistical analysis [125].
We identified eight studies where the inhaler training interventions (including such aspects as physical demonstration, technique labels, and written action plans) led to an improvement in inhaler technique and also a significant increase in disease control, (seven in asthma [39, 83, 84, 87, 94, 96, 111], and one in COPD [88]) while 4 studies reported that their intervention significantly improved disease outcomes or reduced hospital admission frequency, but did not measure inhaler error frequency [98, 105, 116, 117]. Two further studies reported that training significantly improved technique and outcomes in asthma, but not in COPD patients [68, 104]. Eight studies reported no significant relationship between poor inhaler technique or errors with asthma control [34, 40, 58, 59, 70, 86, 89, 126].
Association between quality of life and inhaler errors
Seven of the 114 studies examined any association between QoL and inhaler errors: three in asthma, two in COPD and two in a mixed population.
A significant improvement in QoL was reported in three studies, following interventions which improved inhalation technique [84, 88, 91]. Basheti observed a significant correlation between improvement in DPI technique and improvement in asthma-related QoL following a pharmacist-led training intervention [84]. Goris reported significant improvements in QoL according to the St. George’s Respiratory Questionnaire (SGRQ) in all domains of QoL following intervention (aided by a movie and leaflet) in pMDI and DPI technique in COPD patients [88]. Maazuddin reported a pharmacist-led intervention led to significant improvements in the SGRQ outcomes in patients with COPD for pMDI and aerosol based devices including, Autohaler® and Evohaler®, but not for the three DPIs Revolizer®, Rotahaler® and Starhaler® [91].
A further study by Plaza reported a clinically significant increase in Mini Asthma Quality of Life Questionnaire scores among patients receiving a repeated training intervention (including development of a personalised action plan) delivered by a professional educator, physician or nurse, but the inhaler error frequency was not captured [98].
In contrast, an RCT by Hesselink found no significant impact on QoL in asthma and COPD (measured using the Quality-of-Life for Respiratory Illness Questionnaire) following a family practice assistant intervention (involving a structured consultation and use of checklist), although a significant improvement in inhaler technique was recorded [89]. An observational, retrospective study by Takemura reported unchanged SGRQ scores in asthma patients following intervention at regular intervals of at least 6 months by certified participants in a community-pharmacist educational program [103]. A further study by Pothirat captured a non-significant relationship between inhaler errors and poor quality of life, as judged by the by COPD Assessment Test (CAT) [34].
Economic models investigating the costs associated with inhaler errors
Our analysis identified eight studies [127,128,129,130,131,132,133,134,135], of which one was reported both in manuscript and abstract form [127, 128].
Roggeri reported a modelling study conducted in Italy and calculated the increased healthcare resource use by asthma or COPD patients making one or more critical inhaler error and showed this was associated with an additional yearly cost of €44,104 (asthma) or €23,444 (COPD) per 100 patients [127, 128]. Contextualising this for COPD, 100 patients making at least one inhaler error would require 11.5 additional hospitalisations, 13 emergency room visits, 19.5 courses of antimicrobials, and 47 courses of oral corticosteroids, compared to 100 patients not making any critical errors. Corresponding figures for 100 asthma patients were 19 hospitalisations, 26.5 emergency room visits, 4.5 antimicrobial courses and 21.5 oral corticosteroid courses [127, 128].
Bijos modelled the impact of poor inhaler technique on healthcare resource use in Poland, and concluded that misuse of inhaled corticosteroid and long-acting beta agonist fixed-dose combinations resulted in an annual loss of 378 million PLN (€91.1 million) in direct costs and 20.4 million PLN (€4.9 million) in indirect productivity, costs across asthma and COPD [129].
Torvinen calculated the effect on disease outcomes and the economic impact of a new DPI inhaler reported to reduce inhalation errors through innovative inhaler characteristics, and showed a potential saving of €57.78 million, based on a 10.1% rate of uptake among 701,983 patients with persistent asthma or COPD in Italy when switching to the new device from their existing DPI inhalers of Turbuhaler® or Diskus®, by year 5 of the model [130].
In the UK, Lewis considered the impact of inhaler errors on the economic burden of asthma and COPD with inhaled corticosteroid/long-acting beta-agonist (ICS/LABA) fixed-dose combinations [131]. The authors estimated that 366,000 of the 1.3 million persistent asthma/COPD patients within the UK have poor inhalation technique, and that this was associated with 11.8% (£16.2 million) of unscheduled health care events per year [131].
In a further study, Lewis estimated the additional resource use due to poor inhalation technique in Spain, and calculated a loss of €11.54 million due to unscheduled healthcare events among 563,562 asthma and COPD patients using Turbuhaler® or Accuhaler®. [132] Two similar economic models considered the impact of improved inhalation technique in asthma and COPD and in the UK and Sweden, and concluded that improved technique could save £3.5 million in the UK through reducing the number of unscheduled health events (assuming an update of 25% in years 4 and 5 of the model), and SEK285.4 million (€31.2 million) in Sweden by reducing the number of lost working days [133, 134].
Of note, four out of the 9 studies were related to the same device utilised in studies sponsored by the same company within a year of each other using the same health economic model employing a device switch approach to the study design [130, 132,133,134].
Conversely, a real world study in COPD (n = 108) conducted in Colombia reported that making inhaler errors was associated with a minor increase in monthly cost per patient ($146.9, versus $142.2 for other patients) [135].
Interestingly, no economics-focused studies on a US population were captured.
Generic issues identified
As previously mentioned, several types of inconsistency or heterogeneity between captured studies were seen during the review – each of which made the analysis of the data challenging.
The inconsistency in defining critical errors versus normal errors makes drawing conclusions on associations difficult, as errors were considered critical or non-critical by different researchers using different definitions; this is an important issue identified throughout the systematic review.
Furthermore, as differing checklists were used, containing differing numbers and descriptions of errors, error frequencies are likely not completely comparable between studies. In addition, “poor technique” was defined differently by different researchers, who commonly used differing thresholds for labelling a patient’s technique as incorrect or poor [55, 56].
In addition, although disease outcomes were captured using known measures of control, the variety of different measures used does make it more difficult to draw firm conclusions on the association between error frequency and asthma control.
Discussion
The aim of our article was to define ‘critical’ inhaler errors and their impact on health outcomes and resource use; and by doing so, to bring to the attention of physicians the importance of the inhaler device in their daily prescribing in the management of patients with asthma and COPD. Indeed, both GINA and GOLD now highlight the critical importance of assessing inhaler technique to guide appropriate inhaler prescribing, with a concerted drive to educate professionals and patients about the real impact of inhaler errors on the patients’ disease control, as well as on the financial economics of societal health.
To our knowledge this is the first formally registered evidence-based systematic review with a priori clearly formulated questions that documents the wide discrepancies within the literature regarding definitions and descriptions of inhaler errors and their classification as either ‘critical’ or ‘non-critical’. Previous reviews such as that by Basheti et al. focusing on inhaler error checklists have approached these issues [136], although in a different context.
Astonishingly, we observed 299 different descriptions of critical inhaler errors. Even for the same inhaler device type, different terminology was used between different study authors to describe the same inhaler error, and this may contribute to the confusion observed in clinical practice with regards to best inhaler practice and the limitations in determining associations with inhaler errors [8]. This heterogeneity and lack of consensus fundamentally hampers the ability to interpret studies with respect to the impact of inhaler errors. Indeed, the different definitions of critical error could be a contributing factor to extremely different conclusions even with the same inhaler device type; as exemplified in the Melani study where MDI users were significantly less likely to commit critical errors relative to DPI users [10], in contrast to the Batterink study where MDI users were most likely to make critical errors [25].
The lack of consensus between researchers extends to the use of differing inhaler technique checklists. As the checklists used are not standardized, even within individual inhaler device types, comparing error rates between or within inhaler device types is unfeasible. Future research can and should adopt more consistent inhaler technique checklists, as the manufacturers’ instructions are available to form a basis for a checklist in almost all cases.
We observed several important factors, including older age, education status, lack of previous inhaler instruction, and lower socioeconomic class, which were all associated with high inhaler error frequency. In addition, inhaler technique interventions were found to decrease error frequency, and have positive impacts on disease and patient outcomes, as has previously been described in the literature by Basheti et al. [137].
However these findings were not reflected in all studies, likely due to differences in study design and populations. For example, both interventional and observational studies were included, there were different inhaler devices included (i.e. pMDI or DPI), and wide ranging population sizes (between 46 and 6512 individuals), thereby limiting our ability to directly compare the results.
Interestingly, a significant association with error frequency was found for some comorbidities that are known to be strongly correlated with age, such as obesity, heart disease, or cognitive impairment [48, 79, 80]; but despite this, only around a third of studies that examined age itself reported a significant association with error frequency.
Our systematic review identified studies showing an association between inhaler errors and poor asthma control and COPD disease stability. This is in line with a recent individual study that has demonstrated that inhaler errors affect drug delivery [138]. Sulaiman showed in a laboratory environment that deliberately making certain inhaler errors led to a reduced amount of drug reaching the bloodstream [138]. However, the limited quantity of disclosed research in this area may suggest that the term “critical” is being overused, with only a weak basis for categorising errors as such.
In a recent real-world study by Molimard in 2935 patients an increased risk of COPD exacerbation among patients who made a critical inhaler error, was confirmed [139]. A further study by Price determined that the error of “insufficient respiratory effort” was associated with increased asthma exacerbation rate, as well as decreased control in general [140].
Importantly, we identified eight economic models which linked inhaler errors to economic burden, of which one study by Roggeri demonstrated a specific link between critical errors and resource use, leading to an excess cost of many thousands of Euros per 100 patients making critical errors [127, 128]. Indeed, recently Lewis and colleagues showed that poor inhalation technique led to approximately ¾ billion euros in direct and indirect costs for just two DPI inhalers used over 1 year [18].
Previous literature has also demonstrated that poor disease outcomes are linked with worsened QoL and increased resource use and economic burden through increased physician consultation time and lost productivity (Additional file 1: Table S3) [141,142,143,144,145,146]. Therefore, the issue of inhaler errors is important to address due to the downstream effects on patients, healthcare systems and society.
Our findings clearly illustrate inhaler technique can be affected by the level of instruction from HCPs. It is therefore important to interpret clinical trial results with caution, given that their controlled environment (where all patients are instructed in inhaler use) may not be representative of clinical practice in real life. This issue is especially important in the context of different inhaler devices that may have ergonomic designs and functions, as raised by Scichilone et al. in a 2015 review [147]. The key message here is that in day-to-day practice, it may be an efficient strategy to provide patients at higher risk of errors with additional specifically tailored in-depth support with their inhaler use, to ensure they are confident with the correct technique.
Greater attention is clearly needed on the routine review of inhaler technique in the patient population as a whole, as a recent study by Sanchis reported rates of common inhaler errors to be static over a period of several decades [11], and data also show that despite optimally prescribed inhaled therapy, levels of asthma control and COPD disease stability remain poor [18, 145].
In comparison with a previously published systematic review only on DPI inhaler errors, our review encompasses a wider range of device types including the most commonly used inhaler device, the pMDI [14]. Whilst Lavorini et al. included data on critical errors and provided a definition of a critical error, their study focused on the incidence of errors and the possible implications for clinical effectiveness of inhalers [14]. A key strength of our review is that it integrates the link between inhaler errors and disease outcomes and QoL, and provides a systematic overview of how these critical inhaler errors are being assessed and measured.
Direct comparisons and synthesis of the data were challenging due to mixed methodologies (such as observational cross-sectional, or interventional cross-over designs, and designs intended for descriptive or qualitative analysis), different patient populations, and varied endpoints. Yet, despite these differences we observed clear trends in our data. However, due to the vast differences between studies, this review did not examine clinical outcomes by device, but this is an important area for future research.
Furthermore, only a handful of the reviewed studies directly addressed patient outcomes and the economic burden of inhaler errors. Therefore, further research and potential health-economic modelling to understand the relationship between inhaler technique and disease outcomes, and the subsequent impact on societal healthcare systems, is vitally required.
Although the present study shows associations between inhaler errors and patient outcomes through a review of chronic obstructive respiratory diseases as a whole, future research may be able to probe further into the two diseases (asthma and COPD). For example, the generally older age, poor prognosis and comorbidities of COPD patients may influence the degree to which their QoL is increased by improvements in technique and control [148]. The substantially higher prevalence of comorbidities among COPD patients, relative to asthma patients, also likely impacts inhaler technique and patient QoL [148].
With the variety of definitions identified in our review, difficulties arise in determining whether a particular inhaler type is inherently more vulnerable to critical inhaler errors. Consistent use of our proposed definition and categorization by all researchers internationally would transform this area of research and greatly facilitate quantitative and objective comparison between devices, providing a clearer indication of the associated error rates. This would revolutionise everyday clinical practice, where reliable comparisons of error rates would greatly help physicians and aid informed treatment decisions, ensuring the most appropriate device is prescribed for the individual patient with clear implications for personalised patient management. Further research into the association of patient characteristics with error rate could examine “health literacy”, a patient’s insight into their own treatment and health system, and determine if poor knowledge is a risk factor for poor technique [115, 149,150,151].
It is clear that inhaler errors have an effect on disease outcomes, and ultimately patient outcomes and economic burden. This in turn will have an impact on overall disease management and affect not only patients but also the wider healthcare system. These findings are increasingly important given the plethora of devices available to HCPs and patients, and highlight the importance of inhaler mastery in managing and treating asthma and COPD.
There is increasing evidence to suggest that correct inhaler technique (mastery) is fundamental for effective therapy, and that inhaler device type and mastery play important roles in improving adherence, clinical outcomes, quality of life, and use of healthcare resources. Evidence suggests that prescribers should consider patients’ mastery of technique (or lack thereof) and ease of use before changing the dose of inhaled medications, switching to a different inhaler, or adding other treatments to the regimen of patients with poorly controlled asthma. Recent international asthma guidelines highlight the importance of testing and ensuring mastery, alongside checking adherence, before increasing or changing therapy.
Conclusions
In conclusion, the multitude of definitions cited within the literature indicates that there is an urgent need for a consensus in the way in which critical (and non-critical) inhaler errors are defined. We propose defining a critical inhaler error as an action or inaction that in itself would have a definite detrimental impact on the delivery of the drug to the lung, in contrast to a non-critical error which we would define as an action or inaction that in combination with other factors may, or may not, contribute to ineffective delivery of the drug to the lung.
We advocate that there is a real need for an independent international panel of inhalation experts to collectively determine, through evidence and consensus, the definitions of critical and non-critical inhaler errors. If done for each device type, this would demystify the current confusion within the respiratory community.
We also propose that future studies classify individual errors into categories such as inhalation manoeuvre, dose preparation, inhaler handling, device-specific or generic, in order to make comparison and analysis simpler in order to ultimately help healthcare professionals help their patients.
Abbreviations
- ACQ :
-
Asthma Control Questionnaire
- ACT:
-
Asthma Control Test
- ATAQ:
-
Asthma Therapy Assessment Questionnaire
- BDI:
-
Baseline Dyspnoea Index
- CAT:
-
COPD Assessment Test
- CI:
-
Confidence interval
- COPD:
-
Chronic obstructive pulmonary disease
- DPI:
-
Dry-powder inhaler
- GINA :
-
Global Initiative for Asthma
- GOLD:
-
Global Initiative for Chronic Obstructive Lung Disease
- GP:
-
General Practitioner
- HCP:
-
Healthcare provider
- ICS:
-
Inhaled corticosteroid
- LABA:
-
Long-acting beta agonist
- MDI:
-
Metered-dose inhaler
- mMRC:
-
Modified Medical Research Council (questionnaire)
- pMDI:
-
Pressurized metered-dose inhaler
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- QoL:
-
quality of life
- RCT:
-
Randomised controlled trial
- SGRQ:
-
St George’s Respiratory Questionnaire
References
-
Gregory KL, Elliott D, Dunne P. Guide to aerosol delivery devices for physicians, nurses, pharmacists and other health care professionals [https://www.aarc.org/wp-content/uploads/2014/08/aerosol_guide_pro.pdf] Accessed: 10 Nov 2015.
-
Pritchard JN. Industry guidance for the selection of a delivery system for the development of novel respiratory products. Expert Opin Drug Deliv. 2015;12:1755–65.
Article
PubMed
CASGoogle Scholar
-
Lavorini F, Usmani OS. Correct inhalation technique is critical in achieving good asthma control. Prim Care Respir J. 2013;22:385–6.
Article
PubMedGoogle Scholar
-
Wright J, Brocklebank D, Ram F. Inhaler devices for the treatment of asthma and chronic obstructive airways disease (COPD). Qual Saf Health Care. 2002;11:376–82.
Article
CAS
PubMed
PubMed CentralGoogle Scholar
-
Price D, Marshall J, Turner R. Inhaler use in five european countries: analysis of sales data from Q4 2005 to Q4 2011. Value Health. 2012;15:A-PMD92.
Google Scholar
-
Price D, Roche N, Christian Virchow J, Burden A, Ali M, Chisholm A, Lee AJ, Hillyer EV, von Ziegenweidt J. Device type and real-world effectiveness of asthma combination therapy: an observational study. Respir Med. 2011;105:1457–66.
Article
PubMedGoogle Scholar
-
Lavorini F, Fontana GA, Usmani OS. New inhaler devices — the good, the bad and the ugly. Respiration. 2014;88:3–15.
Article
PubMedGoogle Scholar
-
Haughney J, Price D, Barnes N, Virchow J, Roche N, Chrystyn H. Choosing inhaler devices for people with asthma: current knowledge and outstanding research needs. Respir Med. 2010;3:125–31.
Google Scholar
-
Molimard M, Raherison C, Lignot S, Depont F, Abouelfath A, Moore N. Assessment of handling of inhaler devices in real life: an observational study in 3811 patients in primary care. J Aerosol Med. 2003;16:249–54.
Article
CAS
PubMedGoogle Scholar
-
Melani AS, Bonavia M, Cilenti V, Cinti C, Lodi M, Martucci P, Serra M, Scichilone N, Sestini P, Aliani M, Neri M. Inhaler mishandling remains common in real life and is associated with reduced disease control. Respir Med. 2011;105:930–8.
Article
PubMedGoogle Scholar
-
Sanchis J, Gich I, Pedersen S. Systematic review of errors in inhaler use: has patient technique improved over time? Chest. 2016;150:394–406.
Article
PubMedGoogle Scholar
-
Molimard M, Raherison C, Lignot S, Balestra A, Lamarque S, Chartier A, Droz-Perroteau C, Lassalle R, Moore N, Girodet PO. Chronic obstructive pulmonary disease exacerbation and inhaler device handling: real-life assessment of 2935 patients. Eur Respir J. 2017;49. doi:10.1183/13993003.01794-2016.
-
Al-Showair RA, Tarsin WY, Assi KH, Pearson SB, Chrystyn H. Can all patients with COPD use the correct inhalation flow with all inhalers and does training help? Respir Med. 2007;101:2395–401.
Article
PubMedGoogle Scholar
-
Lavorini F, Magnan A, Christophe Dubus J, Voshaar T, Corbetta L, Broeders M, Dekhuijzen R, Sanchis J, Viejo JL, Barnes P, et al. Effect of incorrect use of dry powder inhalers on management of patients with asthma and COPD. Respir Med. 2008;102:593–604.
Article
PubMedGoogle Scholar
-
Price D, Bosnic-Anticevich S, Briggs A, Chrystyn H, Rand C, Scheuch G, Bousquet J. Inhaler competence in asthma: common errors, barriers to use and recommended solutions. Respir Med. 2013;107:37–46.
Article
CAS
PubMedGoogle Scholar
-
van der Palen J, Klein JJ, Kerkhoff AH, van Herwaarden CL, Seydel ER. Evaluation of the long-term effectiveness of three instruction modes for inhaling medicines. Patient Educ Couns. 1997;32:S87–95.
Article
CAS
PubMedGoogle Scholar
-
Price DB, Roman-Rodriguez M, RB MQ, Bosnic-Anticevich S, Carter V, Gruffydd-Jones K, Haughney J, Henrichsen S, Hutton C, Infantino A, et al. Inhaler errors in the CRITIKAL study: type, frequency, and association with asthma outcomes. J Allergy Clin Immunol Pract. 2017;5:1071–1081.e1079.
Article
PubMedGoogle Scholar
-
Lewis A, Torvinen S, Dekhuijzen PN, Chrystyn H, Watson AT, Blackney M, Plich A. The economic burden of asthma and chronic obstructive pulmonary disease and the impact of poor inhalation technique with commonly prescribed dry powder inhalers in three European countries. BMC Health Serv Res. 2016;16:251.
Article
CAS
PubMed
PubMed CentralGoogle Scholar
-
Global initiative for chronic obstructive lung disease: pocket guide to COPD diagnosis, management and prevention [http://goldcopd.org/wp-content/uploads/2016/12/wms-GOLD-2017-Pocket-Guide.pdf] Accessed: 26 May 2017.
-
Global initiative for asthma: pocket guide for asthma management and prevention [http://ginasthma.org/2017-pocket-guide-for-asthma-management-and-prevention/] Accessed: 25 July 2017.
-
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. Br Med J. 2009;339:b2700.
-
IMS Health: IMS MIDAS Q4 MAT 2016, EU5. 2016.
Google Scholar
-
Lavorini F, Corrigan CJ, Barnes PJ, Dekhuijzen PR, Levy ML, Pedersen S, Roche N, Vincken W, Crompton GK. Aerosol drug management improvement team: retail sales of inhalation devices in European countries: so much for a global policy. Respir Med. 2011;105:1099–103.
Article
CAS
PubMedGoogle Scholar
-
Basheti IA, Qunaibi E, Bosnic-Anticevich SZ, Armour CL, Khater S, Omar M, Reddel HK. User error with diskus and turbuhaler by asthma patients and pharmacists in Jordan and Australia. Respir Care. 2011;56:1916–23.
Article
PubMedGoogle Scholar
-
Batterink J, Dahri K, Aulakh A, Rempel C. Evaluation of the use of inhaled medications by hospital inpatients with chronic obstructive pulmonary disease. Can J Hosp Pharm. 2012;65:111–8.
PubMed
PubMed CentralGoogle Scholar
-
Deerojanawong J, Na Sakolnakorn VP, Prapphal N, Hanrutakorn C, Sritippayawan S. Evaluation of metered-dose inhaler administration technique among asthmatic children and their caregivers in Thailand. Asian Pac J Allergy Immunol. 2009;27:87–93.
PubMed
Google Scholar
-
Van Der Palen J, Van Der Valk P, Goosens M, Groothuis-Oudshoorn K, Brusse-Keizer M. A randomised cross-over trial investigating the ease of use and preference of two dry powder inhalers in patients with asthma or chronic obstructive pulmonary disease. Expert Opin Drug Deliv. 2013;10:1171–8.
Article
PubMedGoogle Scholar
-
Van Der Palen J, Ginko T, Kroker A, Van Der Valk P, Goosens M, Padulles L, Seoane B, Rekeda L, Garcia Gil E. Preference, satisfaction and errors with two dry powder inhalers in patients with COPD. Expert Opin Drug Deliv. 2013;10:1023–31.
Article
PubMedGoogle Scholar
-
Voshaar T, Spinola M, Linnane P, Campanini A, Lock D, Lafratta A, Scuri M, Ronca B, Melani AS. Comparing usability of NEXThaler with other inhaled corticosteroid/long-acting beta2-agonist fixed combination dry powder inhalers in asthma patients. J Aerosol Med Pulm Drug Deliv. 2014;27:363–70.
Article
CAS
PubMed
PubMed CentralGoogle Scholar
-
Wieshammer S, Dreyhaupt J. Dry powder inhalers: which factors determine the frequency of handling errors? Respiration. 2008;75:18–25.
Article
PubMedGoogle Scholar
-
Capstick T, Clifton I, Morgan J, Silcock J, Blenkinsopp A. Inhaler technique: an unmet need in patients with difficult asthma? Eur Respir J. 2013;42:A-4893.
Google Scholar
-
Nama S, Percival M, Harris M, Nolan-Neylan S, Sivakumaran P, Sriram K, Harland K. Evaluation of inhaler technique and medication adherence in COPD patients. Respirology. 2014;19:A-TP146.
Google Scholar
-
Vanderman AJ, Moss JM, Bailey JC, Melnyk SD, Brown JN. Inhaler misuse in an older adult population. Consult Pharm. 2015;30:92–100.
Article
PubMedGoogle Scholar
-
Pothirat C, Chaiwong W, Phetsuk N, Pisalthanapuna S, Chetsadaphan N, Choomuang W. Evaluating inhaler use technique in COPD patients. Int J Chron Obstruct Pulmon Dis. 2015;10:1291–8.
Article
CAS
PubMed
PubMed CentralGoogle Scholar
-
Madkour A, Galal I. Do Egyptian patients use their inhalers correctly? A checklist auditing for inhalation devices usage techniques. Egyptian J Chest Dis Tuberculosis. 2015;64:497–504.
Article
Google Scholar
-
Ozturk C, Aldag Y. Evaluation and importance of different types of inhaler device use in patients with chronic obstructive lung disease (COPD). Respirology. 2015;20(S3):A-471.
-
Chrystyn H, Price DB, Molimard M, Haughney J, Bosnic-Anticevich S, Lavorini F, Efthimiou J, Shan D, Sims E, Burden A. Comparison of serious inhaler technique errors made by device-naïve patients using three different dry powder inhalers: a randomised, crossover, open-label study. BMC Pulm Med. 2016;16:12.
Article
PubMed
PubMed Central
CASGoogle Scholar
-
Coelho ACC, Souza-Machado A, Leite M, Almeida P, Castro L, Cruz CS, Stelmach R, Cruz AA. Use of inhaler devices and asthma control in severe asthma patients at a referral center in the city of Salvador, Brazil. J Bras Pneumol. 2011;37:720–8.
Article
PubMedGoogle Scholar
-
Giraud V, Allaert FA, Roche N. Inhaler technique and asthma: Feasability and acceptability of training by pharmacists. Respir Med. 2011;105:1815–22.
Article
PubMedGoogle Scholar
-
Hagmolen of ten Have W, van de Berg NJ, Bindels PJ, van Aalderen WM, van der Palen J. Assessment of inhalation technique in children in general practice: increased risk of incorrect performance with new device. J Asthma. 2008;45:67–71.
Article
PubMedGoogle Scholar
-
Mehuys E, Boussery K, Adriaens E, van Bortel L, De Bolle L, van Tongelen I, Remon JP, Brusselle G. COPD management in primary care: an observational, community pharmacy-based study. Ann Pharmacother. 2010;44:257–66.
Article
PubMedGoogle Scholar
-
Molimard M, Gros VL. Impact of patient-related factors on asthma control. J Asthma. 2008;45:109–13.
Article
PubMedGoogle Scholar
-
Rajan S, Gogtay J. Ease-of-use, preference, confidence, and satisfaction with Revolizer, a novel dry powder inhaler, in an Indian population. Lung India. 2014;31:366–74.
Article
PubMed
PubMed CentralGoogle Scholar
-
Rootmensen G, Van Keimpema AR, Jansen HM, De Haan RJ. Predictors of incorrect inhalation technique in patients with asthma or COPD. Am J Respir Crit Care Med. 2010;181:A-3812.
Google Scholar
-
Schulte M, Osseiran K, Betz R, Wencker M, Brand P, Meyer T, Haidl P. Handling of and preferences for available dry powder inhaler systems by patients with asthma and COPD. J Aerosol Med Pulm Drug Deliv. 2008;21:321–8.
Article
CAS
PubMedGoogle Scholar
-
Van Der Palen J, Ginko T, Kroker A, Van Der Valk P, Goosens M, Padulles L, Seoane B, Rekeda L, Gil EG. Comparison of the preference, satisfaction, and critical errors made with Genuair and Handihaler in patients with COPD. Chest. 2012;142:A-717A.
Article
Google Scholar
-
Molimard M. How to achieve good compliance and adherence with inhalation therapy. Curr Med Res Opin. 2005;21:S33–7.
Article
PubMedGoogle Scholar
-
Westerik JA, Carter V, Chrystyn H, Burden A, Thompson SL, Ryan D, Gruffydd-Jones K, Haughney J, Roche N, Lavorini F, et al. Characteristics of patients making serious inhaler errors with a dry powder inhaler and association with asthma-related events in a primary care setting. J Asthma. 2016;53:321–9.
Article
PubMed
PubMed CentralGoogle Scholar
-
Chrystyn H, Bosnic-Anticevich S, Roche N, Molimard M, Haughney J, Lavorini F, Shan D, Sims E, Burden A, Ashton VL. Prevalence of serious post-training inhaler technique errors made by device-naïve patients using three different dry powder inhalers (DPIs). Eur Respir J. 2015;46:A-P3927.
Google Scholar
-
Thomas M, Van der Palen J, Chrystyn H, Sharma R, Imber V, Zhu C-Q, Barnes N. Inhaler errors and preference: a comparison of two multi-dose powder asthma inhalers. Respirology. 2015;20:A-573.
Article
Google Scholar
-
Li H, Chen Y, Zhang Z, Dong X, Zhang G, Zhang H. Handling of diskus dry powder inhaler in Chinese chronic obstructive pulmonary disease patients. J Aerosol Med Pulm Drug Deliv. 2014;27:219–27.
Article
PubMedGoogle Scholar
-
Melani AS, Canessa P, Coloretti I, Deangelis G, Detullio R, Del Donno M, Giacobbe R, Scarlato I, Serafini A, Barbato N, et al. Inhaler mishandling is very common in patients with chronic airflow obstruction and long-term home nebuliser use. Respir Med. 2012;106:668–76.
Article
PubMedGoogle Scholar
-
Capanoglu M, Dibek Misirlioglu E, Toyran M, Civelek E, Kocabas CN. Evaluation of inhaler technique, adherence to therapy and their effect on disease control among children with asthma using metered dose or dry powder inhalers. J Asthma. 2015;52:838–45.
Article
PubMed
CASGoogle Scholar
-
Pascual S, Feimer J, De Soyza A, Sauleda Roig J, Haughney J, Padulles L, Seoane B, Rekeda L, Ribera A, Chrystyn H. Preference, satisfaction and critical errors with Genuair and Breezhaler inhalers in patients with COPD: a randomised, cross-over, multicentre study. NPJ Prim Care Respir Med. 2015;25:15018.
Article
PubMed
PubMed CentralGoogle Scholar
-
Bryant L, Bang C, Chew C, Hee Baik S, Wiseman D. Adequacy of inhaler technique used by people with asthma or chronic obstructive pulmonary disease. JJ Prim Health Care. 2013;5:191–8.
Google Scholar
-
Dalcin PTR, Grutcki DM, Laporte PP, de Lima PB, Menegotto SM, Pereira RP. Factors related to the incorrect use of inhalers by asthma patients. J Bras Pneumol. 2014;40:13–20.
Article
PubMed CentralGoogle Scholar
-
Giraud V, Allaert FA, Magnan A. A prospective observational study of patient training in use of the autohaler inhaler device: the sirocco study. Eur Rev Med Pharmacol Sci. 2011;15:563–70.
CAS
PubMedGoogle Scholar
-
Harnett CM, Hunt EB, Bowen BR, O’Connell OJ, Edgeworth DM, Mitchell P, Eustace JA, Henry MT, Kennedy MP, Plant BJ, Murphy DM. A study to assess inhaler technique and its potential impact on asthma control in patients attending an asthma clinic. J Asthma. 2014;51:440–5.
Article
CAS
PubMedGoogle Scholar
-
Loh LC, Teng CL, Teh PN, Koh CN, Vijayasingham P, Thayaparan T. Metered-dose inhaler technique in asthmatic patients — a revisit of the Malaysian scene. Med J Malaysia. 2004;59:335–41.
CAS
PubMedGoogle Scholar
-
Chorao P, Pereira AM, Fonseca JA. Inhaler devices in asthma and COPD — an assessment of inhaler technique and patient preferences. Respir Med. 2014;108:968–75.
Article
PubMedGoogle Scholar
-
Hammerlein A, Muller U, Schulz M. Pharmacist-led intervention study to improve inhalation technique in asthma and COPD patients. J Eval Clin Pract. 2011;17:61–70.
Article
PubMedGoogle Scholar
-
Al-Hassan MI. Assessment of inhaler technique in patients attending a chest hospital in Riyadh City. Int J Pharmacol. 2009;5:232–5.
Article
Google Scholar
-
Komase Y, Asako A, Kobayashi A, Sharma R. Ease-of-use preference for the ELLIPTA dry powder inhaler over a commonly used single-dose capsule dry powder inhaler by inhalation device-naive Japanese volunteers aged 40 years or older. Int J COPD. 2014;9:1365–75.
Article
Google Scholar
-
Ozturk C, Kaya A, Bilgin C, Yucesoy L, Ikidag B, Demirel M, Baslilar S, Saylan B, Senol T, Aganoglu S, et al. Evaluation of inhaler technique and patient satisfaction with fixed-combination budesonide/formoterol dry-powder inhaler in chronic obstructive pulmonary disease (COPD): data on real-life clinical practice in Turkey. Tuberk Toraks. 2012;60:301–13.
Article
PubMedGoogle Scholar
-
Nolan-Neylan S, Harris M, Harland K, Sriram K. Evaluation of inhaler technique in hospitalised COPD patients. Respirology. 2015;20:A-P002.
Google Scholar
-
Lee SM, Chang YS, Kim CW, Kim TB, Kim SH, Kwon YE, Lee JM, Lee SK, Jeong JW, Park JW, et al. Skills in handling Turbuhaler, Diskus, and pressurized metered-dose inhaler in Korean asthmatic patients. Allergy Asthma Immunol Res. 2010;3:46–52.
Article
PubMed
PubMed CentralGoogle Scholar
-
Al-Jahdali H, Ahmed A, Al-Harbi A, Khan M, Baharoon S, Bin Salih S, Halwani R, Al-Muhsen S. Improper inhaler technique is associated with poor asthma control and frequent emergency department visits. Allergy Asthma Clin Immunol. 2013;9:8.
Article
PubMed
PubMed CentralGoogle Scholar
-
Maricoto T, Rodrigues LV, Teixeira G, Valente C, Andrade L, Saraiva A. Assessment of inhalation technique in clinical and functional control of asthma and chronic obstructive pulmonary disease. Acta Med Port. 2015;28:702–7.
Article
PubMedGoogle Scholar
-
Manriquez P, Acuna AM, Munoz L, Reyes A. Study of inhaler technique in asthma patients: differences between pediatric and adult patients. J Bras Pneumol. 2015;41:405–9.
Article
PubMed
PubMed CentralGoogle Scholar
-
Sriram KB, Percival M. Suboptimal inhaler medication adherence and incorrect technique are common among chronic obstructive pulmonary disease patients. Chron Respir Dis. 2015;13:13–22.
Article
PubMed
PubMed CentralGoogle Scholar
-
Buset EMN, Liaaen ED, Roth K, Blix HS. Inhalation technique in hospitalized asthma and COPD patients: should patients be regularly assessed before discharge? Int J Clin Pharm. 2015;37:A-16.
Google Scholar
-
Cayo-Quiñe A, Martínez-Vargas V, Bustamante-Voysest R, Piscoya A, Alberca Y: Incorrect use of metered-dose inhalers in adult patients at a hospital in Callao, Peru, 2014: cross-sectional study. Medwave 2014, 15:e6163-e6163.
-
Sangita P, Gharti KP, Laxman B. Assessment of inhalation techniques in COPD patients using metered-dose inhaler and Rotahaler at a tertiary care hospital in Nepal. Int Res J Pharm. 2015;6:288–93.
Article
Google Scholar
-
Villamil-Osorio M, Medina L, Pernett L, Restrepo SM, Nino G, Rodriguez-Martinez C. Assessment of inhalation technique and predictors of poor inhalation technique in a population of asthmatic children. J Aerosol Med Pulm Drug Deliv. 2015;191:A-3370.
Google Scholar
-
Udwadia ZZ, Kathar S, Shah HD, Pandey K, Rastogi S, Mullerpattan J. Who will teach the teachers: an analysis of the inhaler technique of Indian patients and health care providers. Am J Res Crit Care Med. 2013;187:A5026.
-
Turan P, Itil O, Turan M. Factors effecting inhaler technique in COPD. Am J Res Crit Care Med. 2014;189:A-6000.
-
Wu H, Thomas L, Bime C. An assessment of inhaler technique among patients with chronic obstructive airway diseases in a health professional shortage area. Am Philos Soc. 2013;187:A4208.
-
Baddar S, Jayakrishnan B, Al-Rawas OA. Asthma control: importance of compliance and inhaler technique assessments. J Asthma. 2014;51:429–34.
Article
PubMedGoogle Scholar
-
Sadowski C, Banh H, Cor K, Cave A. Inhaler device technique in community-dwelling older adults. Canadian Journal of. Hosp Pharm. 2013;66(4):269.
Google Scholar
-
Camilleri K, Balzan M, Bardon MP, Schembri E, Sullivan M, Mifsud S, Muscat D, Asciaq R, Montefort S. Predictors of good inhaler technique in asthma and COPD. Eur Respir J. 2015;46:A-P3928.
Google Scholar
-
Ganguly A, Das A, Roy A, Adhikari A, Banerjee J, Sen S. Study of proper use of inhalational devices by bronchial asthma or copd patients attending a tertiary care hospital. J Clin Diagn Res. 2014;8:HC04–7.
PubMed
PubMed CentralGoogle Scholar
-
Khassawneh BY, Al-Ali MK, Alzoubi KH, Batarseh MZ, Al-Safi SA, Sharara AM, Alnasr HM. Handling of inhaler devices in actual pulmonary practice: metered-dose inhaler versus dry powder inhalers. Respir Care. 2008;53:324–8.
PubMed
Google Scholar
-
Barthwal MS, Katoch CDS, Marwah V. Impact of optimal asthma education programme on asthma morbidity, inhalation technique and asthma knowledge. J Assoc Physicians India. 2009;57:574–9.
CAS
PubMedGoogle Scholar
-
Basheti IA, Armour CL, Bosnic-Anticevich SZ, Reddel HK. Evaluation of a novel educational strategy, including inhaler-based reminder labels, to improve asthma inhaler technique. Patient Educ Couns. 2008;72:26–33.
Article
PubMedGoogle Scholar
-
Burkhart PV, Rayens MK, Bowman RK. An evaluation of children’s metered-dose inhaler technique for asthma medications. Nurs Clin N Am. 2005;40:167–82.
Article
Google Scholar
-
Carpenter DM, Lee C, Blalock SJ, Weaver M, Reuland D, Coyne-Beasley T, Mooneyham R, Loughlin C, Geryk LL, Sleath BL. Using videos to teach children inhaler technique: a pilot randomized controlled trial. J Asthma. 2015;52:81–7.
Article
PubMedGoogle Scholar
-
Garcia-Cardenas V, Sabater-Hernandez D, Kenny P, Martinez-Martinez F, Faus MJ, Benrimoj SI. Effect of a pharmacist intervention on asthma control. A cluster randomised trial. Respir Med. 2013;107:1346–55.
Article
PubMedGoogle Scholar
-
Goris S, Tasci S, Elmali F. The effects of training on inhaler technique and quality of life in patients with COPD. J Aerosol Med Pulm Drug Deliv. 2013;26:336–44.
Article
PubMed
CASGoogle Scholar
-
Hesselink AE, Penninx BWJH, Van Der Windt DAWM, Van Duin BJ, De Vries P, Twisk JWR, Bouter LM, Van Eijk JTM. Effectiveness of an education programme by a general practice assistant for asthma and COPD patients: results from a randomised controlled trial. Patient Educ Couns. 2004;55:121–8.
Article
PubMedGoogle Scholar
-
Levy ML, Hardwell A, McKnight E, Holmes J. Asthma patients’ inability to use a pressurised metered-dose inhaler (pMDI) correctly correlates with poor asthma control as defined by the global initiative for asthma (GINA) strategy: a retrospective analysis. Prim Care Res J. 2013;22:406–11.
Google Scholar
-
Maazuddin M, Hazari MAH, Hasan A, Javeedullah M, Nasir Mohiuddin M, Baig MMA. Training in the use of inhalation devices and respiratory improvement in asthma and COPD patients: a before-after experimental study. Pharmanest. 2014;5:2314–20.
Google Scholar
-
Minai BA, Martin JE, Cohn RC. Results of a physician and respiratory therapist collaborative effort to improve long-term metered-dose inhaler technique in a pediatric asthma clinic. Respir Care. 2004;49:600–5.
PubMed
Google Scholar
-
Van Der Palen J, Eijsvogel MM, Kuipers BF, Schipper M, Vermue NA. Comparison of the Diskus inhaler and the Handihaler regarding preference and ease of use. J Aerosol Med. 2007;20:38–44.
Article
PubMedGoogle Scholar
-
Yildiz F, Erbagci A, Demirel YS, Akcali SD, Ekici A, Dursunoglu N, Ediger D, Erdinc M, Cemri SC, Kalyoncu AF, et al. Importance of inhaler device use status in the control of asthma in adults: the asthma inhaler treatment study. Respir Care. 2014;59:223–30.
Article
PubMedGoogle Scholar
-
Elgendy MO, Abdelrahim ME, Eldin RS. Potential benefit of repeated MDI inhalation technique counselling for patients with asthma. Eur J Hosp Pharm. 2015;22:318–22.
Article
Google Scholar
-
Grover C, Goel N, Armour C, Van Asperen P, Gaur S, Moles R, Saini B. Medication education program for Indian children with asthma: a feasibility study. Niger J Clin Pract. 2016;19:76–84.
Article
CAS
PubMedGoogle Scholar
-
Kuna P, Kupryś-Lipińska I, Dębowski T. Control of asthma in adults treated with beclomethasone and formoterol in extrafine particle formulation in a real-life setting in Poland: the CASPER noninterventional, observational trial. Pol Arch Med Wewn. 2015;125:731–40.
PubMed
Google Scholar
-
Plaza V, Peiró M, Torrejón M, Fletcher M, López-Viña A, Ignacio JM, Quintano JA, Bardagí S, Gich I. A repeated short educational intervention improves asthma control and quality of life. Eur Respir J. 2015;46:1298–307.
Article
CAS
PubMedGoogle Scholar
-
Bell D, Mansfield L, Lomax M, Dissanayake S. Patient handling study of fluticasone propionate/formoterol fumarate pressurized metered-dose inhaler. Respirology. 2014;19:A-O016.
Google Scholar
-
Kuprys-Lipinska I, Wiacek K, Przyrowski R, Kuna P. The educational program on the inhalation technique in a group of patients with asthma and COPD using Aerolizer — the effectiveness and the patients’ satisfaction. J Allergy Clin Immunol. 2011;1:A-443.
Google Scholar
-
Lin HL, Ng SP, Chen CH, Chien SY. Pharmacist-led educational interventions to improve inhalation technique in pediatric asthma patients. Pharmacoepidemiol Drug Saf. 2014;23:A-P414.
Google Scholar
-
Shetty F, Gupta R. Improved MDI inhaler technique observed in adult asthma patients with web based education. Eur Respir J. 2013;42:A-4959.
Google Scholar
-
Takemura M, Mitsui K, Ido M, Koyama M, Matsumoto M, Inoue D, Takamatsu K, Itotani R, Ishitoko M, Suzuki S. Clinical impact of a program to educate community pharmacists in providing proper inhalation technique for asthma patients. Eur Respir J. 2011;38:2845.
-
Maricoto T, Madanelo S, Rodrigues L, Teixeira G, Valente C, Andrade L, Saraiva A. Inhalation technique education and its impact in asthma and COPD. Eur Respir J. 2015;46:A-P5019.
Google Scholar
-
Fernandes L, Mesquita A. Improving asthma control with therapeutic education intervention. Eur Respir J. 2011;38:A-P4997.
Google Scholar
-
Barnestein-Fonseca P, Leiva-Fernández F, Vazquez-Alarcon R, Aguiar-Leiva V, Lobnig-Becerra M, Leiva-Fernández J. Can we improve the inhalation techniques in patients with COPD? Tiepoc study. Value Health. 2015;7:A-PRS10.
Google Scholar
-
Van Der Valk P, Goosens M, Groothuis-Oudshoorn K, Brusse-Keizer M, van der Palen J. Comparing the ease of use, preference and satisfaction of Accuhaler/Diskus and Elpenhaler in patients with asthma or chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187:A2336.
-
Prieto-Centurion V, Bracken NE, Jaffe HA, Hauser J, Norwick L, Krishnan JA, Zaidi F. Reducing avoidable readmissions following COPD exacerbations among US veterans: the importance of teaching appropriate use of respiratory inhalers. Am J Respir Crit Care Med. 2015;191:A6177.
-
Wiacek K, Kuna P, Kuprys-Lipinska I. The clinical effectiveness of the improvement of the inhalation technique in patients using aerolizer-2nd phase of the educational-observational program. American J Res Crit Care Med. 2012:185, A-5625.
-
Lee S-Y, Park H-W, Song W-J, Cho S-H. A multifaceted approach to reduce acute exacerbations in elderly asthmatics. Chest. 2015;148:A-11A.
Article
Google Scholar
-
Ammari W, Al-Hyari N, Obeidat N, Khater M, Sabouba A, Sanders M. Improving paediatrics’ pressurised metered dose inhaler technique and asthma control: inhaler verbal counselling vs. Trainhaler. Thorax. 2015;70:A-P100.
Article
Google Scholar
-
Ronk J, Alarcon L, Loughlin C. Implementing standardized metered-dose-inhaler (MDI) spacer technique checklist for pediatric asthma patients across University of North Carolina (UNC) Children’s hospital. Am J Respir Crit Care Med. 2012;185:A-3359.
Google Scholar
-
Al-Doghim I. Evaluation of inhalation technique of metered dose inhaler (MDI) and dry powder inhaler-Turbuhaler (DPI) among pediatric patients with asthma. J Appl Sci. 2007;9:53–66.
Google Scholar
-
Khan G, Badri P, Parbati T, Anita D, Atul A, Deepak P, Dipendra R, Himal B, Kabita G, Nirmala K. Intervention on inhalation technique of Rotahaler in patients with chronic obstructive pulmonary disease and asthma. Asian J Pharm Sci. 2016;11:81–2.
Article
Google Scholar
-
Alsomali H, Vines DL, Stein BD, EA B: Evaluating the health literacy and effectiveness of written dry powder inhaler instructions in patients diagnosed with chronic obstructive pulmonary disease. Am Assoc Res Care Open Forum 2015, 60:A-2303288.
-
Benjamin JA, Williams R, Bruce K, Jones O, Philips L. A 2 year programme to improve inhaler technique for adult patients with asthma and chronic obstructive pulmonary disease in a welsh university health board. Eur Respir J. 2015;46:A-P3929.
Google Scholar
-
Sulaiman I, MacHale E, Seheult J, D’Arcy S, Rapcan V, Mokoka M, Cushen B, Killane I, Franciosi A, Sahadevan A. Feedback on adherence and inhaler technique using the Inca device: a randomised control trial in severe asthma. Am J Respir Crit Care Med. 2016;193:A-1714.
Google Scholar
-
Thomas M, Van Der Palen J, Chrystyn H, Zhu C, Ghatta S, Svedsater H. Time to achieve correct inhaler use and inhaler preference: a comparison of Ellipta® with three inhaler devices in patients with asthma. Am J Respir Crit Care Med. 2016;193:A-1739.
Google Scholar
-
Van Der Palen J, Thomas M, Chrystyn H, Sharma R, Imber V, Zhu C-Q, Svedsater H. Training and time to achieve correct inhaler use: a comparison between inhalers in patients with COPD. In: AJRCCM conference. San Francisco, CA, US: American Thoracic Society; 2016. p. A-6812.
Google Scholar
-
Juniper EF, O’Byrne PM, Guyatt GH, Ferrie PJ, King DR. Development and validation of a questionnaire to measure asthma control. Eur Respir J. 1999;14:902–7.
Article
CAS
PubMedGoogle Scholar
-
Nathan RA, Sorkness CA, Kosinski M, Schatz M, Li JT, Marcus P, Murray JJ, Pendergraft TB. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113:59–65.
Article
PubMedGoogle Scholar
-
Azevedo P, Correia de Sousa J, Bousquet J, Bugalho-Almeida A, Del Giacco SR, Demoly P, Haahtela T, Jacinto T, Garcia-Larsen V, van der Molen T, et al. Control of allergic rhinitis and asthma test (CARAT): dissemination and applications in primary care. Prim Care Res J. 2013;22:112–6.
Google Scholar
-
Skinner EA, Diette GB, Algatt-Bergstrom PJ, Nguyen TT, Clark RD, Markson LE, AW W. The asthma therapy assessment questionnaire (ATAQ) for children and adolescents. Dis Manag. 2004;7:305–13.
Article
PubMedGoogle Scholar
-
Murphy KR, Zeiger RS, Kosinski M, Chipps B, Mellon M, Schatz M, Lampl K, Hanlon JT, Ramachandran S. Test for respiratory and asthma control in kids (TRACK): a caregiver-completed questionnaire for preschool-aged children. J Allergy Clin Immunol. 2009;123:833–9. e839
Article
PubMedGoogle Scholar
-
Groot EP, Kreggemeijer WJ, Brand PL. Getting the basics right resolves most cases of uncontrolled and problematic asthma. Acta Paediatr. 2015;104:916–21.
Article
PubMedGoogle Scholar
-
Zaidi S, Williams J, Monaghan T, Burhan H, Main N. Inhaler Technique: Does Poor Technique Mean More Admissions? Am J Respir Crit Care Med. 2012;185:A-3333.
Google Scholar
-
Roggeri A, Micheletto C, Boarino S, Inzillo V, Roggeri DP. Potential economic impact of inhalation errors due to device switch in patients with chronic obstructive pulmonary disease and asthma. Value Health. 2015;18:A-PMD147.
Google Scholar
-
Roggeri A, Micheletto C, Roggeri DP. Inhalation errors due to device switch in patients with chronic obstructive pulmonary disease and asthma: critical health and economic issues. Int J Chron Obstruct Pulmon Dis. 2016;11:597–602.
Article
PubMed
PubMed CentralGoogle Scholar
-
Bijos P, Kaczynski J, Torvinen S, Lenarczyk E, Wrona W, Plich A, Lewis A, Blackney M. Clinical and economic burden of asthma and chronic obstructive pulmonary disease (COPD) in Poland: estimated impact of poor inhalation technique with inhaled corticosteroid and long-acting beta agonist fixed-dose combinations. Value Health. 2015;18:A-PRS34.
Article
Google Scholar
-
Torvinen S, Nicolai J, Pulimeno S, di Nola L, Bruno G, Colombo G, Di Matteo S, Valentino M, Lewis A, Blackney M. The budget impact of Duoresp® Spiromax® compared with commonly prescribed dry powder inhalers for the management of asthma and chronic obstructive pulmonary disease in Italy: estimated impact of inhalation technique. Value Health. 2015;18:A-PRS16.
Google Scholar
-
Lewis A, Blackney M, Torvinen S, Plich A. Clinical and economic burden of asthma and chronic obstructive pulmonary disease in the UK: impact of critical inhaler errors with inhaled corticosteroid + long-acting beta agonist fixed-dose combinations. Value Health. 2014;17:A-PRS30.
Article
Google Scholar
-
Lewis A, Blackney M, Garcia BL, Sánchez-de la Rosa R, Torvinen S, Plich A. The potential for improved inhalation technique with Duoresp® Spiromax®(budesonide+formoterol fumarate dihydrate) compared with commonly prescribed dry powder inhalers for the management of asthma and chronic obstructive pulmonary disease in Spain: estimated impact on number and cost of unscheduled healthcare events. Value Health. 2015;18:A-PMD37.
Google Scholar
-
Lewis A, Blackney M, Torvinen S, Lindqvist F, Safioti G, Grundstrom J, Polyzoi M, Plich A. The potential societal cost benefits of improved inhalation technique with Duoresp Spiromax (budesonide + formoterol fumarate dihydrate) compared with Symbicort Turbuhaler for the management of asthma and chronic obstructive pulmonary disease in sweden. Value Health. 2014;17:A-PRS62.
Article
Google Scholar
-
Lewis A, Blackney M, Torvinen S, Holmes J, Osborne M, Dale J, Chandler S, Plich A. The budget impact of Duoresp Spiromax (budesonide + formoterol fumarate dihydrate) compared with Symbicort Turbohaler for the management of asthma and chronic obstructive pulmonary disease in the United Kingdom: impact on health care costs and inhalation technique. Value Health. 2014;17:A-PRS19.
Article
Google Scholar
-
Estrada J, Restrepo A, Serna J, Herrera R, Arrieta J, Segura A. Impact of a pharmacotherapeutic follow-up program on the cost-month-patient, stratified by risk-pharmacological type. Value Health. 2015;18:A-PRS14.
Google Scholar
-
Basheti I, Bosnic-Anticevich S, Armour C, Reddel H. Checklists for powder inhaler technique: a review and recommendations. Respir Care. 2014;59:1140–54.
Article
PubMedGoogle Scholar
-
Basheti IA, Reddel HK, Armour CL, Bosnic-Anticevich SZ. Improved asthma outcomes with a simple inhaler technique intervention by community pharmacists. J Allergy Clin Immunol. 2007;119:1537–8.
Article
PubMedGoogle Scholar
-
Sulaiman I, Seheult J, Sadasivuni N, Cushen B, Mokoka M, Costello R. Inhaler technique errors have an impact on drug delivery. Am J Respir Crit Care Med. 2016;193:A-1715.
Google Scholar
-
Molimard M, Raherison C, Lignot S, Balestra A, Lamarque S, Chartier A, Droz-Perroteau C, Lassalle R, Moore N, Girodet P-O. Chronic obstructive pulmonary disease exacerbation and inhaler device handling: real-life assessment of 2935 patients. Eur Respir J. 2016;49
-
Price DB, Roman-Rodriguez M, McQueen RB, Bosnic-Anticevich S, Carter V, Gruffydd-Jones K, Haughney J, Henrichsen S, Hutton C, Infantino A, et al. Inhaler errors in the CRITIKAL study: type, frequency, and association with asthma outcomes. J Allergy Clin Immunol Pract. 2017;5:1071–1081.e1079.
Article
PubMedGoogle Scholar
-
Williams SA, Wagner S, Kannan H, Bolge SC. The association between asthma control and health care utilization, work productivity loss and health-related quality of life. J Occup Environ Med. 2009;51:780–5.
Article
PubMedGoogle Scholar
-
Vervloet D, Williams A, Lloyd A, Clark T. Costs of managing asthma as defined by a derived asthma control TestTM score in seven European countries. Eur Respir Rev. 2006;15:17–23.
Article
Google Scholar
-
Szende A, Svensson K, Ståhl E, Meszaros A, Berta GY. Psychometric and utility-based measures of health status of asthmatic patients with different disease control level. PharmacoEconomics. 2004;22:537–47.
Article
PubMedGoogle Scholar
-
Doz M, Chouaid C, Com-Ruelle L, Calvo E, Brosa M, Robert J, Decuypere L, Pribil C, Huerta A, Detournay B. The association between asthma control, health care costs, and quality of life in France and Spain. BMC Pulm Med. 2013;13:15.
Article
PubMed
PubMed CentralGoogle Scholar
-
Demoly P, Annunziata K, Gubba E, Adamek L. Repeated cross-sectional survey of patient-reported asthma control in Europe in the past 5 years. Eur Respir Rev. 2012;21:66–74.
Article
CAS
PubMedGoogle Scholar
-
Jha A, Heron L, Marshall J, Dunlop W. Device handling errors and the impact on quality of life and health care resource use in asthmatic patients. Value Health. 2014;17:A-PRS64.
Google Scholar
-
Scichilone N, Benfante A, Bocchino M, Braido F, Paggiaro P, Papi A, Santus P, Sanduzzi A. Which factors affect the choice of the inhaler in chronic obstructive respiratory diseases? Pulm Pharmacol Ther. 2015;31:63–7.
Article
CAS
PubMedGoogle Scholar
-
Lavorini F, Mannini C, Chellini E, Fontana GA. Optimising inhaled pharmacotherapy for elderly patients with chronic obstructive pulmonary disease: the importance of delivery devices. Drugs Aging. 2016;33:461–73.
Article
CAS
PubMedGoogle Scholar
-
Perez L, Morales K, Huang J, Ndicu G, Han X, Klusaritz H, Localio A, Apter AJ. Aspects of asthma self-management: inhaler technique, ability to access (navigate) health care, and inhaled steroid knowledge are correlated. Am J Res Crit Care Med. 2016;193:A6426.
-
Kiser K, Jonas D, Warner Z, Scanlon K, Shilliday BB, DeWalt DA. A randomized controlled trial of a literacy-sensitive self-management intervention for chronic obstructive pulmonary disease patients. The. J Gen Intern Med. 2012;27:190–5.
Article
PubMedGoogle Scholar
-
Paasche-Orlow MK, Riekert KA, Bilderback A, Chanmugam A, Hill P, Rand CS, Brancati FL, Krishnan JA. Tailored education may reduce health literacy disparities in asthma self-management. Am J Respir Crit Care Med. 2005;172:980–6.
Article
PubMed
PubMed CentralGoogle Scholar
-
Al Zabadi H, El Sharif N. Factors associated with frequent emergency room attendance by asthma patients in Palestine. Int J Tuberc Lung Dis. 2007;11:920–7.
CAS
PubMedGoogle Scholar
-
Azouz W, Chetcuti P, Hosker H, Saralaya D, Chrystyn H. Objective measurement of inhalation profiles in patients using metered dose inhalers (MDIs). Eur Respir J. 2011;38:A-838.
Google Scholar
-
Baddar S, Al-Rawas O. What is missing in the asthma control test? The relationship between compliance, inhaler technique and level of control. Eur Respir J. 2012;40:A-P513.
Article
Google Scholar
-
Bilal M, Ahmed A, Shah AR, Mirza HA, Anwar AK, Zaidi SBH. Prevalence of the correct technique of using an inhaler among asthmatic patients reporting in tertiary care hospitals of Rawalpindi, Pakistan. J Allergy Clin Immunol. 2012;1:A-159.
Google Scholar
-
Caliskaner Z, Ozturk C, Pekcan S, Yilmaz O, Ozturk S, Ceylan E, Can C, Sener O, Turay U, Ersoy R. The «extreme» errors in inhaler device use: data from the INTEDA-1 study. In: Allergy; 2011. p. 369–70.
Google Scholar
-
Chrystyn H, Pascual S, Feimer J, De Soyza A, Sauleda Roig J, Haughney J, Padulles L, Seoane B, Rekeda L, Ribera A. Preference, satisfaction and critical errors with Genuair and Breezhaler in patients with COPD. Eur Respir J. 2014;44:A-P928.
Google Scholar
-
Deering B, MacCormack N, Kerrigan K, D’Arcy S, Costello RW. Adherence to inhalers after discharge from hospital following an exacerbation of COPD. Ir J Med Sci. 2013;182:S458.
Google Scholar
-
Hass C, Engdahl K, Albert W, Setyawan J, Mateo N. Patient preferences and perceived ease of use in inhaler features: Genuair vs other inhalers. Chest. 2010;138:A-484.
Article
Google Scholar
-
Herscher M, Ray M, Busse PJ, Wolf MS, Wisnivesky JP, Federman A. Characteristics and outcomes of older adults with early versus late onset asthma. Am J Respir Crit Care Med. 2014;189:A-1359.
Article
CASGoogle Scholar
-
Leiva-Fernandez F, Leiva-Fernandez J, Porcel-Martin C, Prados-Torres D, Garcia-Ruiz AJ, Barnestein-Fonseca P. How do patients with chronic obstructive pulmonary disease (COPD) use their inhalers? Common mistakes. Tecepoc study. Value Health. 2013;16:A-PRS45.
Google Scholar
-
Mazankova D, Mendelova I, Saloun J. Identification of error rate in using inhalation devices by asthmatic patients. Int J Clin Pharm. 2013;35(6):1279–80.
Google Scholar
-
Muhammad I, Haque AS, Muhammad N, Khan JA. Real life perspective in outpatient asthma treatment at a tertiary care center of Pakistan. Respirology. 2009;14:A-PD 10-09.
Google Scholar
-
Santos JC, Silveira BF, Rizzatti F. Knowledge of and technique for using inhalation devices among asthma and COPD patients. Am J Res Crit Care Med. 2014;A-4656
-
Souza M, Meneghini A, Ferraz E, Vianna E, Borges M. Knowledge of and technique for using inhalation devices among asthma patients and COPD patients. J Bras Pneumol. 2009;35:824–31.
Article
PubMedGoogle Scholar
-
Tarsin W, Alshamli I, Soussi M. Preference of the inhaler device and assessment of the technique among the asthmatic and COPD patients. Eur Respir J. 2011;38:A-3981.
Google Scholar
-
Williams J, Mault S, Garner N, Burhan H, Zaidi S. Breaking down bad inhaler technique: device specific advice. Am J Respir Crit Care Med. 2012;185:A-3332.
Google Scholar
Download references
Acknowledgements
We would like to thank Alison Saunders, Iván Viejo Viejo and Rebecca Forster for their support in quality checking and co-ordinating this manuscript and Robin Wyn for editorial assistance.
Funding
Funding was provided by Mundipharma International Ltd. to Adelphi Values Ltd. to support this research and the writing of the manuscript. No financial payment was provided to the individual authors of the review.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Trademark
® DISKHALER, DISKUS and ROTAHALER are registered trademarks of Glaxo Group Limited.
® ACCUHALER and EVOHALER are registered trademarks (in the European Union) of Glaxo Group Limited.
® REVOLIZER is a registered trade mark (in the United States) of Cipla Limited.
® AUTOHALER is a registered trade mark of 3 M Company.
® STARHALER is a registered trade mark (in India) of Sun Pharma Laboratories Limited.
® TURBUHALER is a registered trade mark (in the European Union) of AstraZeneca AB.
® HANDIHALER and HandiHaler are registered trademarks of Boehringer Ingelheim Pharma GmbH & Co. KG.
® AEROLIZER is a registered trade mark of Novartis AG.
® GENUAIR is a registered trade mark of AstraZeneca AB.
® BREEZHALER is a registered trade mark (in the European Union) of Novartis AG.
® ELPENHALER is a registered trade mark of Elpen Pharmaceutical Co. Inc.
® CYCLOHALER is a registered trade mark (in the European Union) of Pharmachemie B.V.
® EASI-BREATHE is a registered trade mark (in the European Union) of Norton Healthcare Limited.
® PULVINAL is a registered trade mark (in the European Union) of Chiesi Farmaceutici S.p.A.
® PULMOJET is a registered trade mark (in the European Union) of Sanofi S.A.
Author information
Authors and Affiliations
-
Airway Disease, NHLI, Imperial College London & Royal Brompton Hospital, Dovehouse Street, London, SW3 6LY, UK
Omar Sharif Usmani
-
Department of Experimental and Clinical Medicine, Careggi University Hospital, Florence, Italy
Federico Lavorini
-
Mundipharma International Limited, Cambridge Science Park, Cambridge, CB4 0AB, UK
Jonathan Marshall & William Christopher Nigel Dunlop
-
Adelphi Values, Adelphi Mill, Macclesfield, Cheshire, SK10 5JB, UK
Louise Heron & Emily Farrington
-
Radboud University Medical Center, Nijmegen, Netherlands
Richard Dekhuijzen
Authors
- Omar Sharif Usmani
You can also search for this author in
PubMed Google Scholar - Federico Lavorini
You can also search for this author in
PubMed Google Scholar - Jonathan Marshall
You can also search for this author in
PubMed Google Scholar - William Christopher Nigel Dunlop
You can also search for this author in
PubMed Google Scholar - Louise Heron
You can also search for this author in
PubMed Google Scholar - Emily Farrington
You can also search for this author in
PubMed Google Scholar - Richard Dekhuijzen
You can also search for this author in
PubMed Google Scholar
Contributions
All authors have contributed equally to the analysis, review, writing and finalisation of this manuscript. All authors have read and approved the final manuscript.
Corresponding author
Correspondence to
Omar Sharif Usmani.
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
In the last 5 years, Omar S. Usmani and/or his department received research grants, unrestricted educational grants, and/or fees for lectures and advisory board meetings from Aerocrine, Astra Zeneca, Boehringer Ingelheim, Chiesi, Cipla, Edmond Pharma, GlaxoSmithKline, Napp, Mundipharma International, Prosonix, Sandoz, Takeda, Zentiva.
In the last 5 years, Federico Lavorini received fees for lectures and advisory board meetings from Astra Zeneca, Boehringer Ingelheim, Chiesi, Cipla, Menarini International, TEVA, Zentiva.
In the last 3 years, Richard Dekhuijzen and/or his department received research grants, unrestricted educational grants, and/or fees for lectures and advisory board meetings from AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Mundipharma International, Novartis, Takeda and Teva.
William Dunlop and Jonathan Marshall are employees of Mundipharma International Ltd., United Kingdom.
Emily Farrington and Louise Heron are employees of Adelphi Values Ltd., UK. Adelphi Values Ltd. received funding from Mundipharma International Ltd. to support this research.
The authors do not report any conflict of interest with regards to the contents of this study other than those stated.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
One supplementary file is associated with this manuscript: “Online Resource – Critical handling errors in asthma and COPD: A systematic review of impact on health outcomes”. This contains: search strategies and details of the analysis conducted within this literature review (Table S1); a breakdown of grouped critical errors described in the literature for different inhaler device types (Table S2); summaries of pre-existing known publications that show associations between poor disease control, economic burden and poor QoL (Table S3); definitions of a ‘critical’ error provided by studies captured within the literature review (Table S4). This file is named: “Critical handling errors data supplement update v8_0”. (DOCX 588 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Reprints and Permissions
About this article
Cite this article
Usmani, O.S., Lavorini, F., Marshall, J. et al. Critical inhaler errors in asthma and COPD: a systematic review of impact on health outcomes.
Respir Res 19, 10 (2018). https://doi.org/10.1186/s12931-017-0710-y
Download citation
-
Received: 07 September 2017
-
Accepted: 21 December 2017
-
Published: 16 January 2018
-
DOI: https://doi.org/10.1186/s12931-017-0710-y
Keywords
- Obstructive lung diseases
- Adherence
- Errors
- Aerosols
- Inhalers
- Review
- Open Access
- Published: 16 January 2018
- Federico Lavorini2,
- Jonathan Marshall3,
- William Christopher Nigel Dunlop3,
- Louise Heron4,
- Emily Farrington4 &
- …
- Richard Dekhuijzen5
Respiratory Research
volume 19, Article number: 10 (2018)
Cite this article
-
22k Accesses
-
153 Citations
-
129 Altmetric
-
Metrics details
Abstract
Background
Inhaled drug delivery is the cornerstone treatment for asthma and chronic obstructive pulmonary disease (COPD). However, use of inhaler devices can be challenging, potentially leading to critical errors in handling that can significantly reduce drug delivery to the lungs and effectiveness of treatment.
Methods
A systematic review was conducted to define ‘critical’ errors and their impact on health outcomes and resource use between 2004 and 2016, using key search terms for inhaler errors in asthma and COPD (Search-1) and associated health-economic and patient burden (Search-2).
Results
Search-1 identified 62 manuscripts, 47 abstracts, and 5 conference proceedings (n = 114 total). Search-2 identified 9 studies. We observed 299 descriptions of critical error. Age, education status, previous inhaler instruction, comorbidities and socioeconomic status were associated with worse handling error frequency. A significant association was found between inhaler errors and poor disease outcomes (exacerbations), and greater health-economic burden.
Conclusions
We have shown wide variations in how critical errors are defined, and the evidence shows an important association between inhaler errors and worsened health outcomes. Given the negative impact diminished disease outcomes impose on resource use, our findings highlight the importance of achieving optimal inhaler technique, and a need for a consensus on defining critical and non-critical errors.
Background
Inhaled drug delivery is the cornerstone of therapy for the treatment of obstructive chronic airway diseases, such as asthma and chronic obstructive pulmonary disease (COPD) [1]. The most common devices used to administer aerosolized medication in day-to-day respiratory practice are the pressurized metered-dose inhaler (pMDI) and the dry powder inhaler (DPI). pMDIs are most often prescribed [2], but patients need to inhale correctly and coordinate breathing and actuation to ensure effective drug delivery [3,4,5,6]. In contrast, DPIs are breath-actuated, with most devices relying on a rapid and powerful inhalation manoeuvre for drug delivery, which can be particularly problematic for patients who struggle to inhale forcefully [6].
Recent advances in inhaler technologies have seen an explosion in the number of devices [7]. This plethora of devices, however, has led to confusion in their use amongst health-care providers (HCPs) and patients, who may not properly understand how to use inhalers [8]. Indeed, mastering an inhaler device involves correct preparation and handling of the device before inhalation, and an optimal inhalation technique; an error in any step of this process may lead to inadequate drug delivery to the lungs.
There is no one ‘perfect device’ and several studies have shown that inhaler technique errors made by patients with asthma and COPD are common in real life with both pMDIs and DPIs despite advances in inhaler device technology [3, 9,10,11,12]. Although study results vary, estimates of those making inhaler errors range up to 90% of patients irrespective of the device type used [13, 14]. Most importantly, it is vital to distinguish between ‘critical’ (sometimes defined as ‘essential’ or ‘crucial’) errors, which are likely to significantly impair the delivery of adequate medication to the lungs, and ‘non-critical’ errors, which are likely to result in a reduced amount of drug reaching the lungs compared with that attained using the correct technique [15, 16].
A recent major cross-sectional study of asthma patients has compared inhaler technique data with data on disease control, in order to determine which errors are most associated with poor health outcomes [17]. The results of this may provide the most coherent basis for defining and identifying critical errors; however, progress towards fully elucidating these errors is slow.
The societal and health-economic burden of poor inhaler technique is increasingly being recognised [10]. Worryingly, in three countries (the UK, Spain and Sweden) poor inhaler technique accounted for over €750 million in direct and indirect costs in 2015, for the two most commonly used DPIs [18]. These cost data, together with the increasing prevalence of obstructive lung diseases and restriction in healthcare spending is propagating the imperative need for inhaler competency (that is, correct and effective inhaler use) [15].
Recent global position documents from the Global Initiative for Asthma (GINA) and Global Initiative for Chronic Obstructive Lung Disease (GOLD) both give significant prominence to assessing and correcting poor inhalation technique before escalating drug therapy [19, 20].
Price et al. proposed the need for policy change and research focusing on current gaps in knowledge: specifically on the association between device errors and health economic and clinical outcomes, and on the patient characteristics associated with a higher frequency of errors [15]. Indeed, clinicians must recognise that the device itself and its characteristics are at least equally as important as the prescribed drug; and that in future, the choice of drug compound may be considered to be of secondary importance [3].
The aim of this study was to define ‘critical’ errors and their impact on health outcomes and resource use between 2004 and 2016. This was accomplished through systematically reviewing the scientific literature on inhaler errors made by patients when using pMDIs and DPIs, and the approaches used to assess them — exploring the relationships between inhaler errors, disease outcomes, quality of life, and healthcare resource use, and associations between patient characteristics and inhaler errors. Given the striking variety of inhaler errors reported in the literature [11], this paper focuses on critical errors, as these are most likely to have a health impact.
Methods
Overview
This systematic review was undertaken in accordance with the methodological and reporting standards recommended by PRISMA [21], and was registered in the PROSPERO international prospective register of systematic reviews (CRD42016036118). The review consisted of two distinct searches: search-1 focused on definitions and descriptions of critical errors, and search-2 aimed to identify the literature regarding economic models on the cost of critical errors and patient burden (see Additional file 1: Table S1).
Inclusion criteria
Studies from search-1 were included if they reported data on inhaler errors with pMDI and/or DPIs in patients with asthma or COPD, and if they related inhaler technique to disease outcomes or quality of life (QoL). Studies from search-2 were included if they reported data on the patient and/or economic burden of inhaler errors. Soft-mist inhalers and nebulisers were not considered in either search, as pMDIs and DPIs are estimated to make up around 99.8% of the global market share of inhaler devices [22].
Both searches were conducted, reviewed, and each article checked, by two authors (LH, EF) in four online databases (Embase, Medline, EconLIT and Evidence-Based Medicine Reviews), limited to studies published in English between 2004 and May 2016. International conference proceedings from 2013 to 2016 were also scanned (see Additional file 1: Table S1). All the authors reviewed the finalized list of selected articles for approval.
Data extraction
The following data were recorded from each selected article: author and contact details; number of patients; patient characteristics including age, gender, education, comorbidities, socioeconomic class, concurrent device use, and previous instruction; type(s) of inhaler; type(s) of inhaler error(s); definition of critical error(s); type of disease (asthma, COPD, or both); and findings on disease outcomes or QoL.
We grouped the emergent themes into 5 domains in our systematic review; (1) patient characteristics, (2) educational aspects, (3) disease outcomes, (4) quality of life, (5) health economics. This qualitative assessment of the study results allowed results to be reported more clearly, in order to help explore the impact of critical errors on health outcomes and resource use.
When studies were examined for evidence of an association between patient characteristics and presence or rate of inhaler errors, an a priori predefined list of characteristics agreed by consensus between the authors was used to focus analysis. This included: patient age, gender, socioeconomic class, education level, inhaler education, comorbidities, and the number of inhaler devices prescribed at the same time.
Additionally, the reference lists of all retrieved papers were reviewed for any potentially relevant studies, and editorials, commentaries, case studies, letters and opinion pieces were excluded. Studies examining nebuliser inhaler errors or those pooling nebulizer inhaler errors data with data for other inhalers were excluded, as our aim was to assess inhaler devices that administer a single discrete dose. Studies that did not specify inhaler types were included, as it was considered likely that pMDIs and DPIs would have been used, due to these of inhaler types comprising the majority of market share [23]. Descriptive methods were used to analyse data for the associations mentioned above.
Results
Search results
Initially (not including grey literature), Search-1 yielded 114 studies: 62 of these were full-text articles and 52 were abstracts. Of these, five abstracts were identified as having an economics focus and were therefore moved to the results of Search-2 (Fig. 1). Following the addition of five grey literature abstracts, the total yield of Search-1 was again 114 studies.
PRISMA diagram. The database search and analysis in Search-1 initially yielded 114 full-text articles or abstracts; give abstracts were removed and incorporated into the results of Search-2 due to being economics-focused; a further five abstracts were added to Search-1 following the grey literature search. Therefore, the final yield of Search-1 was 114
Full size image
All studies (n = 114) in Search-1 reported inhaler error data on pMDIs with or without spacers, and single- or multiple-dose DPIs (Fig. 2a and b). Study details including population age, respiratory disease, and inhaler device type are presented in Table 1.
a. Journal articles reporting critical inhaler errors for pMDIs and DPIs. Note: percentages are calculated as a proportion of total mentions (n = 105) of each inhaler type by all inhaler error studies. Individual studies may mention more than one inhaler type. b. Journal articles reporting critical inhaler errors for specific DPI device types, both multi-dose (blue) and single-dose (red). Note: percentages are calculated as a proportion of total mentions (n = 65) of all device types by all inhaler error studies. Individual studies may mention more than one inhaler type. c. Studies stating a definition of a critical error, separated into categories. Details of each study and the exact wording used by each are presented in Additional file 1: Table S4. Note: In this figure the term “critical error” refers to both critical errors and critical steps that, when performed incorrectly, constitute critical errors
Full size image
Full size table
Search-2 on the health-economic burden of inhaler errors yielded only one full-text article and three abstracts that fulfilled the inclusion criteria, to which five abstracts from Search-1 were added (Fig. 1).
Definition of critical inhaler errors
Among the 36 studies giving specific examples of ‘critical’ errors, 32 included a definition of ‘critical’ inhaler errors, and the definition itself substantially varied between the studies (Fig. 2c). In most cases, studies did not provide information on the origin of their definition of a critical error; however, where this information was provided, definitions were commonly taken from previous studies, rather than being formulated by the study researchers. Astonishingly, our search yielded 299 descriptions of critical errors across the device types.
The most common definition was an action affecting the lung deposition of inhaled drug, resulting in little or no medicine being inhaled or reaching the lungs (n = 27), where 14 definitions stated a critical error “would” certainly affect inhalation and drug delivery [24,25,26,27,28,29,30,31,32,33,34,35,36,37], and 13 others said a critical error “could” affect these [38,39,40,41,42,43,44,45,46,47,48,49,50]. Conversely, 4 papers defined a critical error in terms of effectiveness: that is, an error that would make aerosol therapy useless [10, 51,52,53]; and Pascual used a combined definition of deposition and effectiveness: that is, “an error that compromised the potential benefit of the treatment, such as impeding drug deposition or the delivery of an insufficient dose” [54].
Surprisingly, only sixty studies (53%) used a checklist to quantify errors and to enable comparisons between devices. However, these checklists were often created by the authors themselves (either taken from previous studies, or were copied from the instructions provided with the inhaler device), without external validation of the checklist itself for each device type. The number of critical errors described varied by device type and by study (Additional file 1: Table S2).
To further compound matters, there were also differences in the descriptions of the actual errors themselves. For example, one DPI error was described in four different ways: two studies mentioned the critical steps which, if not performed, would be errors: “slide lever as far as possible” [42]; “push lever back completely” [27]; and two gave differing terminology for the critical error: “failure to slide the lever until the ‘click’ sound” [51] and “not sliding back the lever until a click is heard” [30]. Similarly, there were also differences in agreement between the authors of the different studies in the categorization of a critical error versus a non-critical error, once again affecting attempts to compare studies and collectively understand the impact of inhaler errors in daily clinical practice. For example, not holding the inhaler upright whilst using a pMDI was referred to as a critical error or step by three studies [39, 42, 44], but Bryant defined it simply as an “error” [55].
While many studies reported associations between characteristics or patient experiences and errors, these did not specify whether associations existed with critical errors specifically, or with all errors.
Effects of patient characteristics on frequency of inhaler errors
Overall, 41 studies of 114 (36%) investigated the effect of predefined patient characteristics on inhaler error frequency (Table 1), with patient age, gender, level of education, number of devices prescribed, and previous inhaler instruction being the most commonly explored factors.
Of 33 studies which examined the effect of patient age [10, 26, 30, 33, 34, 38, 40, 44, 48, 53, 55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77], 29 were in adults and 4 were paediatric. Only twelve studies (36%) reported age to be significantly associated with worsening frequency of inhaler errors [10, 26, 30, 44, 53, 57, 60, 64, 66, 69, 72, 73], whereas 21 studies found no significant association. In 7 studies, older adults were found to make significantly more errors [10, 30, 44, 57, 60, 64, 66]. Of the 4 paediatric studies [26, 40, 53, 74], two reported a significant association between age and frequency of errors: Deerojanawong reported that younger children made errors significantly more frequently [26], while Capanoglu reported the opposite finding: that older children made errors more frequently [53]. Twenty-five studies of 114 (22%) reported on the effects of gender [10, 30, 34, 38, 40, 44, 48, 53, 55, 56, 59,60,61, 63, 65,66,67, 70, 73, 74, 76,77,78,79,80], where 6 studies concluded a significant impact on inhaler error frequency, but the results were contradictory and inconclusive as to whether male or female gender was associated with poor technique [48, 53, 60, 66, 79, 80]. Of the 22 studies that reported a trend between low education and high inhaler error frequency [10, 34, 38, 44, 48, 53, 56, 59,60,61,62, 64,65,66,67, 70, 73,74,75,76, 80, 81], 10 found the association to be statistically significant [10, 34, 48, 53, 56, 60, 62, 66, 73, 80].
Of the 114 articles, 21 studies (18%) explored the relationship between previous inhaler instruction and inhaler error frequency [10, 25, 26, 30, 36, 39, 40, 44, 48, 53, 61, 62, 66,67,68, 71, 72, 74, 76, 80, 81], where 11 studies found previous education or instruction to be significantly related to better inhaler technique [10, 36, 39, 44, 48, 53, 61, 66, 68, 76, 80]. One study by Al-Jahdali reported a significant relationship between ‘lack of education about medication’ and improper device use [67], and two reported that reduced error frequency among previously instructed patients was dependent on device type, where technique improved only in patients using MDI spacer [26] or Diskus or Turbuhaler. [30] Interestingly, a third of studies (n = 7) reported that previous instruction in inhaler use did not significantly affect inhaler technique [25, 40, 62, 71, 72, 74, 81].
Specifically, we noted a statistically significant relationship was reported between increased error frequency and other patient characteristics such as having the presence of two or more comorbidities [56], obesity [48], heart disease [80], cognitive impairment or neuropathy [79], and lower socioeconomic class [56]. There were contradictory results between three studies that reported significant results for whether a higher or lower number of devices prescribed concurrently impacts error frequency [25, 44, 82].
Effects of educational intervention on frequency of inhaler errors
Educational interventions and their relationship to inhaler errors were addressed in 52 articles [27,28,29, 34, 37, 39, 45, 49,50,51, 54, 57,58,59, 61, 83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119], but studies varied in how errors were assessed (the tools used), by whom (the healthcare personnel), and in the duration of intervention. Interventions were undertaken by face-to-face consultation with a variety of HCPs involving physicians (n = 5), nurses (n = 5), paramedics (n = 1), and pharmacists (n = 8). In other studies, a video (n = 5), leaflet instructions (n = 17), or an online program were used (n = 2). Thirty-two studies undertook patient assessments before and after the educational intervention [29, 34, 39, 45, 51, 57,58,59, 61, 83,84,85,86,87,88,89,90,91,92, 94, 95, 97, 100,101,102,103,104, 108, 109, 114, 115]. Where 26 studies positively reported a significant improvement in inhaler technique following the intervention [29, 34, 39, 51, 57, 58, 61, 83,84,85,86,87,88,89, 92, 94, 95, 97, 101, 103, 104, 108, 109, 114, 115].
Analysis of interventions noted that the majority of the pharmacist-led studies, seven of the eight, demonstrated a statistically significant improvement in inhaler technique [39, 61, 84, 87, 91, 101, 103]. Of the five nurse-led interventions [34, 58, 85, 90, 99], three succeeded in significantly improving inhaler technique [34, 58, 85], and two reported a decrease in inhaler error frequency but did not include a statistical analysis [90, 99]. A further six HCP studies reported statistically significant improvements: three physician-led interventions, a physician-and therapist-led study, GP assistant study and a paramedic-led study all reported statistically significant improvements [57, 83, 89, 92, 94, 97]. Four studies with unspecified instructor types reported improvement [45, 51, 95, 102], but only two provided statistical analysis [51, 95]. Of the leaflet-based intervention studies (n = 17) [27,28,29, 37, 45, 49, 50, 54, 88, 93, 104, 106, 107, 112, 115, 118, 119], five compared inhaler technique before and after the intervention, of which four reported a significant improvement in inhaler technique [29, 88, 104, 115].
Association between disease outcomes and inhaler errors
Thirty-six of the 114 studies (Table 1) examined disease outcomes in relation to inhaler errors or inhalation technique (see Table 2 for a summary of available odds ratios). In the assessment of asthma control, the most common measurements were the Asthma Control Questionnaire (ACQ) and Asthma Control Test (ACT) instruments. [120, 121] Other measurements included: the Control of Allergic Rhinitis and Asthma Test [122], Asthma Therapy Assessment Questionnaire [123], Test For Respiratory And Asthma Control In Kids scales [124], frequency of exacerbations, emergency healthcare use, or general classification of patients into levels of disease control using the Global Initiative for Asthma (GINA) criteria. For COPD patients, disease outcomes were measured by: Baseline Dyspnoea Index (BDI), rates of exacerbations, hospitalizations, or by degree of dyspnoea using the modified Medical Research Council (MRC) questionnaire.
Full size table
Our systematic analysis revealed 10 studies observed a higher inhaler error frequency was significantly associated with poor disease outcomes, primarily in asthma (n = 9), but also in asthma and COPD (n = 1) [10, 38, 48, 53, 56, 57, 67, 78, 90, 97, 117]. Molimard reported that using a device incorrectly, irrespective of the type, was associated with an increased Asthma Control Score [42], and in another study by Kuprys-Lipinska and Wiacek, over 94% of patients reported an association between improved DPI technique and better disease outcomes in asthma and COPD; however, no statistical analysis was provided [100, 109]. Groot reported that incorrect inhaler technique with unspecified inhalers was the underlying cause of poor asthma control in 7.8% of its population, but again did not provide statistical analysis [125].
We identified eight studies where the inhaler training interventions (including such aspects as physical demonstration, technique labels, and written action plans) led to an improvement in inhaler technique and also a significant increase in disease control, (seven in asthma [39, 83, 84, 87, 94, 96, 111], and one in COPD [88]) while 4 studies reported that their intervention significantly improved disease outcomes or reduced hospital admission frequency, but did not measure inhaler error frequency [98, 105, 116, 117]. Two further studies reported that training significantly improved technique and outcomes in asthma, but not in COPD patients [68, 104]. Eight studies reported no significant relationship between poor inhaler technique or errors with asthma control [34, 40, 58, 59, 70, 86, 89, 126].
Association between quality of life and inhaler errors
Seven of the 114 studies examined any association between QoL and inhaler errors: three in asthma, two in COPD and two in a mixed population.
A significant improvement in QoL was reported in three studies, following interventions which improved inhalation technique [84, 88, 91]. Basheti observed a significant correlation between improvement in DPI technique and improvement in asthma-related QoL following a pharmacist-led training intervention [84]. Goris reported significant improvements in QoL according to the St. George’s Respiratory Questionnaire (SGRQ) in all domains of QoL following intervention (aided by a movie and leaflet) in pMDI and DPI technique in COPD patients [88]. Maazuddin reported a pharmacist-led intervention led to significant improvements in the SGRQ outcomes in patients with COPD for pMDI and aerosol based devices including, Autohaler® and Evohaler®, but not for the three DPIs Revolizer®, Rotahaler® and Starhaler® [91].
A further study by Plaza reported a clinically significant increase in Mini Asthma Quality of Life Questionnaire scores among patients receiving a repeated training intervention (including development of a personalised action plan) delivered by a professional educator, physician or nurse, but the inhaler error frequency was not captured [98].
In contrast, an RCT by Hesselink found no significant impact on QoL in asthma and COPD (measured using the Quality-of-Life for Respiratory Illness Questionnaire) following a family practice assistant intervention (involving a structured consultation and use of checklist), although a significant improvement in inhaler technique was recorded [89]. An observational, retrospective study by Takemura reported unchanged SGRQ scores in asthma patients following intervention at regular intervals of at least 6 months by certified participants in a community-pharmacist educational program [103]. A further study by Pothirat captured a non-significant relationship between inhaler errors and poor quality of life, as judged by the by COPD Assessment Test (CAT) [34].
Economic models investigating the costs associated with inhaler errors
Our analysis identified eight studies [127,128,129,130,131,132,133,134,135], of which one was reported both in manuscript and abstract form [127, 128].
Roggeri reported a modelling study conducted in Italy and calculated the increased healthcare resource use by asthma or COPD patients making one or more critical inhaler error and showed this was associated with an additional yearly cost of €44,104 (asthma) or €23,444 (COPD) per 100 patients [127, 128]. Contextualising this for COPD, 100 patients making at least one inhaler error would require 11.5 additional hospitalisations, 13 emergency room visits, 19.5 courses of antimicrobials, and 47 courses of oral corticosteroids, compared to 100 patients not making any critical errors. Corresponding figures for 100 asthma patients were 19 hospitalisations, 26.5 emergency room visits, 4.5 antimicrobial courses and 21.5 oral corticosteroid courses [127, 128].
Bijos modelled the impact of poor inhaler technique on healthcare resource use in Poland, and concluded that misuse of inhaled corticosteroid and long-acting beta agonist fixed-dose combinations resulted in an annual loss of 378 million PLN (€91.1 million) in direct costs and 20.4 million PLN (€4.9 million) in indirect productivity, costs across asthma and COPD [129].
Torvinen calculated the effect on disease outcomes and the economic impact of a new DPI inhaler reported to reduce inhalation errors through innovative inhaler characteristics, and showed a potential saving of €57.78 million, based on a 10.1% rate of uptake among 701,983 patients with persistent asthma or COPD in Italy when switching to the new device from their existing DPI inhalers of Turbuhaler® or Diskus®, by year 5 of the model [130].
In the UK, Lewis considered the impact of inhaler errors on the economic burden of asthma and COPD with inhaled corticosteroid/long-acting beta-agonist (ICS/LABA) fixed-dose combinations [131]. The authors estimated that 366,000 of the 1.3 million persistent asthma/COPD patients within the UK have poor inhalation technique, and that this was associated with 11.8% (£16.2 million) of unscheduled health care events per year [131].
In a further study, Lewis estimated the additional resource use due to poor inhalation technique in Spain, and calculated a loss of €11.54 million due to unscheduled healthcare events among 563,562 asthma and COPD patients using Turbuhaler® or Accuhaler®. [132] Two similar economic models considered the impact of improved inhalation technique in asthma and COPD and in the UK and Sweden, and concluded that improved technique could save £3.5 million in the UK through reducing the number of unscheduled health events (assuming an update of 25% in years 4 and 5 of the model), and SEK285.4 million (€31.2 million) in Sweden by reducing the number of lost working days [133, 134].
Of note, four out of the 9 studies were related to the same device utilised in studies sponsored by the same company within a year of each other using the same health economic model employing a device switch approach to the study design [130, 132,133,134].
Conversely, a real world study in COPD (n = 108) conducted in Colombia reported that making inhaler errors was associated with a minor increase in monthly cost per patient ($146.9, versus $142.2 for other patients) [135].
Interestingly, no economics-focused studies on a US population were captured.
Generic issues identified
As previously mentioned, several types of inconsistency or heterogeneity between captured studies were seen during the review – each of which made the analysis of the data challenging.
The inconsistency in defining critical errors versus normal errors makes drawing conclusions on associations difficult, as errors were considered critical or non-critical by different researchers using different definitions; this is an important issue identified throughout the systematic review.
Furthermore, as differing checklists were used, containing differing numbers and descriptions of errors, error frequencies are likely not completely comparable between studies. In addition, “poor technique” was defined differently by different researchers, who commonly used differing thresholds for labelling a patient’s technique as incorrect or poor [55, 56].
In addition, although disease outcomes were captured using known measures of control, the variety of different measures used does make it more difficult to draw firm conclusions on the association between error frequency and asthma control.
Discussion
The aim of our article was to define ‘critical’ inhaler errors and their impact on health outcomes and resource use; and by doing so, to bring to the attention of physicians the importance of the inhaler device in their daily prescribing in the management of patients with asthma and COPD. Indeed, both GINA and GOLD now highlight the critical importance of assessing inhaler technique to guide appropriate inhaler prescribing, with a concerted drive to educate professionals and patients about the real impact of inhaler errors on the patients’ disease control, as well as on the financial economics of societal health.
To our knowledge this is the first formally registered evidence-based systematic review with a priori clearly formulated questions that documents the wide discrepancies within the literature regarding definitions and descriptions of inhaler errors and their classification as either ‘critical’ or ‘non-critical’. Previous reviews such as that by Basheti et al. focusing on inhaler error checklists have approached these issues [136], although in a different context.
Astonishingly, we observed 299 different descriptions of critical inhaler errors. Even for the same inhaler device type, different terminology was used between different study authors to describe the same inhaler error, and this may contribute to the confusion observed in clinical practice with regards to best inhaler practice and the limitations in determining associations with inhaler errors [8]. This heterogeneity and lack of consensus fundamentally hampers the ability to interpret studies with respect to the impact of inhaler errors. Indeed, the different definitions of critical error could be a contributing factor to extremely different conclusions even with the same inhaler device type; as exemplified in the Melani study where MDI users were significantly less likely to commit critical errors relative to DPI users [10], in contrast to the Batterink study where MDI users were most likely to make critical errors [25].
The lack of consensus between researchers extends to the use of differing inhaler technique checklists. As the checklists used are not standardized, even within individual inhaler device types, comparing error rates between or within inhaler device types is unfeasible. Future research can and should adopt more consistent inhaler technique checklists, as the manufacturers’ instructions are available to form a basis for a checklist in almost all cases.
We observed several important factors, including older age, education status, lack of previous inhaler instruction, and lower socioeconomic class, which were all associated with high inhaler error frequency. In addition, inhaler technique interventions were found to decrease error frequency, and have positive impacts on disease and patient outcomes, as has previously been described in the literature by Basheti et al. [137].
However these findings were not reflected in all studies, likely due to differences in study design and populations. For example, both interventional and observational studies were included, there were different inhaler devices included (i.e. pMDI or DPI), and wide ranging population sizes (between 46 and 6512 individuals), thereby limiting our ability to directly compare the results.
Interestingly, a significant association with error frequency was found for some comorbidities that are known to be strongly correlated with age, such as obesity, heart disease, or cognitive impairment [48, 79, 80]; but despite this, only around a third of studies that examined age itself reported a significant association with error frequency.
Our systematic review identified studies showing an association between inhaler errors and poor asthma control and COPD disease stability. This is in line with a recent individual study that has demonstrated that inhaler errors affect drug delivery [138]. Sulaiman showed in a laboratory environment that deliberately making certain inhaler errors led to a reduced amount of drug reaching the bloodstream [138]. However, the limited quantity of disclosed research in this area may suggest that the term “critical” is being overused, with only a weak basis for categorising errors as such.
In a recent real-world study by Molimard in 2935 patients an increased risk of COPD exacerbation among patients who made a critical inhaler error, was confirmed [139]. A further study by Price determined that the error of “insufficient respiratory effort” was associated with increased asthma exacerbation rate, as well as decreased control in general [140].
Importantly, we identified eight economic models which linked inhaler errors to economic burden, of which one study by Roggeri demonstrated a specific link between critical errors and resource use, leading to an excess cost of many thousands of Euros per 100 patients making critical errors [127, 128]. Indeed, recently Lewis and colleagues showed that poor inhalation technique led to approximately ¾ billion euros in direct and indirect costs for just two DPI inhalers used over 1 year [18].
Previous literature has also demonstrated that poor disease outcomes are linked with worsened QoL and increased resource use and economic burden through increased physician consultation time and lost productivity (Additional file 1: Table S3) [141,142,143,144,145,146]. Therefore, the issue of inhaler errors is important to address due to the downstream effects on patients, healthcare systems and society.
Our findings clearly illustrate inhaler technique can be affected by the level of instruction from HCPs. It is therefore important to interpret clinical trial results with caution, given that their controlled environment (where all patients are instructed in inhaler use) may not be representative of clinical practice in real life. This issue is especially important in the context of different inhaler devices that may have ergonomic designs and functions, as raised by Scichilone et al. in a 2015 review [147]. The key message here is that in day-to-day practice, it may be an efficient strategy to provide patients at higher risk of errors with additional specifically tailored in-depth support with their inhaler use, to ensure they are confident with the correct technique.
Greater attention is clearly needed on the routine review of inhaler technique in the patient population as a whole, as a recent study by Sanchis reported rates of common inhaler errors to be static over a period of several decades [11], and data also show that despite optimally prescribed inhaled therapy, levels of asthma control and COPD disease stability remain poor [18, 145].
In comparison with a previously published systematic review only on DPI inhaler errors, our review encompasses a wider range of device types including the most commonly used inhaler device, the pMDI [14]. Whilst Lavorini et al. included data on critical errors and provided a definition of a critical error, their study focused on the incidence of errors and the possible implications for clinical effectiveness of inhalers [14]. A key strength of our review is that it integrates the link between inhaler errors and disease outcomes and QoL, and provides a systematic overview of how these critical inhaler errors are being assessed and measured.
Direct comparisons and synthesis of the data were challenging due to mixed methodologies (such as observational cross-sectional, or interventional cross-over designs, and designs intended for descriptive or qualitative analysis), different patient populations, and varied endpoints. Yet, despite these differences we observed clear trends in our data. However, due to the vast differences between studies, this review did not examine clinical outcomes by device, but this is an important area for future research.
Furthermore, only a handful of the reviewed studies directly addressed patient outcomes and the economic burden of inhaler errors. Therefore, further research and potential health-economic modelling to understand the relationship between inhaler technique and disease outcomes, and the subsequent impact on societal healthcare systems, is vitally required.
Although the present study shows associations between inhaler errors and patient outcomes through a review of chronic obstructive respiratory diseases as a whole, future research may be able to probe further into the two diseases (asthma and COPD). For example, the generally older age, poor prognosis and comorbidities of COPD patients may influence the degree to which their QoL is increased by improvements in technique and control [148]. The substantially higher prevalence of comorbidities among COPD patients, relative to asthma patients, also likely impacts inhaler technique and patient QoL [148].
With the variety of definitions identified in our review, difficulties arise in determining whether a particular inhaler type is inherently more vulnerable to critical inhaler errors. Consistent use of our proposed definition and categorization by all researchers internationally would transform this area of research and greatly facilitate quantitative and objective comparison between devices, providing a clearer indication of the associated error rates. This would revolutionise everyday clinical practice, where reliable comparisons of error rates would greatly help physicians and aid informed treatment decisions, ensuring the most appropriate device is prescribed for the individual patient with clear implications for personalised patient management. Further research into the association of patient characteristics with error rate could examine “health literacy”, a patient’s insight into their own treatment and health system, and determine if poor knowledge is a risk factor for poor technique [115, 149,150,151].
It is clear that inhaler errors have an effect on disease outcomes, and ultimately patient outcomes and economic burden. This in turn will have an impact on overall disease management and affect not only patients but also the wider healthcare system. These findings are increasingly important given the plethora of devices available to HCPs and patients, and highlight the importance of inhaler mastery in managing and treating asthma and COPD.
There is increasing evidence to suggest that correct inhaler technique (mastery) is fundamental for effective therapy, and that inhaler device type and mastery play important roles in improving adherence, clinical outcomes, quality of life, and use of healthcare resources. Evidence suggests that prescribers should consider patients’ mastery of technique (or lack thereof) and ease of use before changing the dose of inhaled medications, switching to a different inhaler, or adding other treatments to the regimen of patients with poorly controlled asthma. Recent international asthma guidelines highlight the importance of testing and ensuring mastery, alongside checking adherence, before increasing or changing therapy.
Conclusions
In conclusion, the multitude of definitions cited within the literature indicates that there is an urgent need for a consensus in the way in which critical (and non-critical) inhaler errors are defined. We propose defining a critical inhaler error as an action or inaction that in itself would have a definite detrimental impact on the delivery of the drug to the lung, in contrast to a non-critical error which we would define as an action or inaction that in combination with other factors may, or may not, contribute to ineffective delivery of the drug to the lung.
We advocate that there is a real need for an independent international panel of inhalation experts to collectively determine, through evidence and consensus, the definitions of critical and non-critical inhaler errors. If done for each device type, this would demystify the current confusion within the respiratory community.
We also propose that future studies classify individual errors into categories such as inhalation manoeuvre, dose preparation, inhaler handling, device-specific or generic, in order to make comparison and analysis simpler in order to ultimately help healthcare professionals help their patients.
Abbreviations
- ACQ :
-
Asthma Control Questionnaire
- ACT:
-
Asthma Control Test
- ATAQ:
-
Asthma Therapy Assessment Questionnaire
- BDI:
-
Baseline Dyspnoea Index
- CAT:
-
COPD Assessment Test
- CI:
-
Confidence interval
- COPD:
-
Chronic obstructive pulmonary disease
- DPI:
-
Dry-powder inhaler
- GINA :
-
Global Initiative for Asthma
- GOLD:
-
Global Initiative for Chronic Obstructive Lung Disease
- GP:
-
General Practitioner
- HCP:
-
Healthcare provider
- ICS:
-
Inhaled corticosteroid
- LABA:
-
Long-acting beta agonist
- MDI:
-
Metered-dose inhaler
- mMRC:
-
Modified Medical Research Council (questionnaire)
- pMDI:
-
Pressurized metered-dose inhaler
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- QoL:
-
quality of life
- RCT:
-
Randomised controlled trial
- SGRQ:
-
St George’s Respiratory Questionnaire
References
-
Gregory KL, Elliott D, Dunne P. Guide to aerosol delivery devices for physicians, nurses, pharmacists and other health care professionals [https://www.aarc.org/wp-content/uploads/2014/08/aerosol_guide_pro.pdf] Accessed: 10 Nov 2015.
-
Pritchard JN. Industry guidance for the selection of a delivery system for the development of novel respiratory products. Expert Opin Drug Deliv. 2015;12:1755–65.
Article
PubMed
CASGoogle Scholar
-
Lavorini F, Usmani OS. Correct inhalation technique is critical in achieving good asthma control. Prim Care Respir J. 2013;22:385–6.
Article
PubMedGoogle Scholar
-
Wright J, Brocklebank D, Ram F. Inhaler devices for the treatment of asthma and chronic obstructive airways disease (COPD). Qual Saf Health Care. 2002;11:376–82.
Article
CAS
PubMed
PubMed CentralGoogle Scholar
-
Price D, Marshall J, Turner R. Inhaler use in five european countries: analysis of sales data from Q4 2005 to Q4 2011. Value Health. 2012;15:A-PMD92.
Google Scholar
-
Price D, Roche N, Christian Virchow J, Burden A, Ali M, Chisholm A, Lee AJ, Hillyer EV, von Ziegenweidt J. Device type and real-world effectiveness of asthma combination therapy: an observational study. Respir Med. 2011;105:1457–66.
Article
PubMedGoogle Scholar
-
Lavorini F, Fontana GA, Usmani OS. New inhaler devices — the good, the bad and the ugly. Respiration. 2014;88:3–15.
Article
PubMedGoogle Scholar
-
Haughney J, Price D, Barnes N, Virchow J, Roche N, Chrystyn H. Choosing inhaler devices for people with asthma: current knowledge and outstanding research needs. Respir Med. 2010;3:125–31.
Google Scholar
-
Molimard M, Raherison C, Lignot S, Depont F, Abouelfath A, Moore N. Assessment of handling of inhaler devices in real life: an observational study in 3811 patients in primary care. J Aerosol Med. 2003;16:249–54.
Article
CAS
PubMedGoogle Scholar
-
Melani AS, Bonavia M, Cilenti V, Cinti C, Lodi M, Martucci P, Serra M, Scichilone N, Sestini P, Aliani M, Neri M. Inhaler mishandling remains common in real life and is associated with reduced disease control. Respir Med. 2011;105:930–8.
Article
PubMedGoogle Scholar
-
Sanchis J, Gich I, Pedersen S. Systematic review of errors in inhaler use: has patient technique improved over time? Chest. 2016;150:394–406.
Article
PubMedGoogle Scholar
-
Molimard M, Raherison C, Lignot S, Balestra A, Lamarque S, Chartier A, Droz-Perroteau C, Lassalle R, Moore N, Girodet PO. Chronic obstructive pulmonary disease exacerbation and inhaler device handling: real-life assessment of 2935 patients. Eur Respir J. 2017;49. doi:10.1183/13993003.01794-2016.
-
Al-Showair RA, Tarsin WY, Assi KH, Pearson SB, Chrystyn H. Can all patients with COPD use the correct inhalation flow with all inhalers and does training help? Respir Med. 2007;101:2395–401.
Article
PubMedGoogle Scholar
-
Lavorini F, Magnan A, Christophe Dubus J, Voshaar T, Corbetta L, Broeders M, Dekhuijzen R, Sanchis J, Viejo JL, Barnes P, et al. Effect of incorrect use of dry powder inhalers on management of patients with asthma and COPD. Respir Med. 2008;102:593–604.
Article
PubMedGoogle Scholar
-
Price D, Bosnic-Anticevich S, Briggs A, Chrystyn H, Rand C, Scheuch G, Bousquet J. Inhaler competence in asthma: common errors, barriers to use and recommended solutions. Respir Med. 2013;107:37–46.
Article
CAS
PubMedGoogle Scholar
-
van der Palen J, Klein JJ, Kerkhoff AH, van Herwaarden CL, Seydel ER. Evaluation of the long-term effectiveness of three instruction modes for inhaling medicines. Patient Educ Couns. 1997;32:S87–95.
Article
CAS
PubMedGoogle Scholar
-
Price DB, Roman-Rodriguez M, RB MQ, Bosnic-Anticevich S, Carter V, Gruffydd-Jones K, Haughney J, Henrichsen S, Hutton C, Infantino A, et al. Inhaler errors in the CRITIKAL study: type, frequency, and association with asthma outcomes. J Allergy Clin Immunol Pract. 2017;5:1071–1081.e1079.
Article
PubMedGoogle Scholar
-
Lewis A, Torvinen S, Dekhuijzen PN, Chrystyn H, Watson AT, Blackney M, Plich A. The economic burden of asthma and chronic obstructive pulmonary disease and the impact of poor inhalation technique with commonly prescribed dry powder inhalers in three European countries. BMC Health Serv Res. 2016;16:251.
Article
CAS
PubMed
PubMed CentralGoogle Scholar
-
Global initiative for chronic obstructive lung disease: pocket guide to COPD diagnosis, management and prevention [http://goldcopd.org/wp-content/uploads/2016/12/wms-GOLD-2017-Pocket-Guide.pdf] Accessed: 26 May 2017.
-
Global initiative for asthma: pocket guide for asthma management and prevention [http://ginasthma.org/2017-pocket-guide-for-asthma-management-and-prevention/] Accessed: 25 July 2017.
-
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. Br Med J. 2009;339:b2700.
-
IMS Health: IMS MIDAS Q4 MAT 2016, EU5. 2016.
Google Scholar
-
Lavorini F, Corrigan CJ, Barnes PJ, Dekhuijzen PR, Levy ML, Pedersen S, Roche N, Vincken W, Crompton GK. Aerosol drug management improvement team: retail sales of inhalation devices in European countries: so much for a global policy. Respir Med. 2011;105:1099–103.
Article
CAS
PubMedGoogle Scholar
-
Basheti IA, Qunaibi E, Bosnic-Anticevich SZ, Armour CL, Khater S, Omar M, Reddel HK. User error with diskus and turbuhaler by asthma patients and pharmacists in Jordan and Australia. Respir Care. 2011;56:1916–23.
Article
PubMedGoogle Scholar
-
Batterink J, Dahri K, Aulakh A, Rempel C. Evaluation of the use of inhaled medications by hospital inpatients with chronic obstructive pulmonary disease. Can J Hosp Pharm. 2012;65:111–8.
PubMed
PubMed CentralGoogle Scholar
-
Deerojanawong J, Na Sakolnakorn VP, Prapphal N, Hanrutakorn C, Sritippayawan S. Evaluation of metered-dose inhaler administration technique among asthmatic children and their caregivers in Thailand. Asian Pac J Allergy Immunol. 2009;27:87–93.
PubMed
Google Scholar
-
Van Der Palen J, Van Der Valk P, Goosens M, Groothuis-Oudshoorn K, Brusse-Keizer M. A randomised cross-over trial investigating the ease of use and preference of two dry powder inhalers in patients with asthma or chronic obstructive pulmonary disease. Expert Opin Drug Deliv. 2013;10:1171–8.
Article
PubMedGoogle Scholar
-
Van Der Palen J, Ginko T, Kroker A, Van Der Valk P, Goosens M, Padulles L, Seoane B, Rekeda L, Garcia Gil E. Preference, satisfaction and errors with two dry powder inhalers in patients with COPD. Expert Opin Drug Deliv. 2013;10:1023–31.
Article
PubMedGoogle Scholar
-
Voshaar T, Spinola M, Linnane P, Campanini A, Lock D, Lafratta A, Scuri M, Ronca B, Melani AS. Comparing usability of NEXThaler with other inhaled corticosteroid/long-acting beta2-agonist fixed combination dry powder inhalers in asthma patients. J Aerosol Med Pulm Drug Deliv. 2014;27:363–70.
Article
CAS
PubMed
PubMed CentralGoogle Scholar
-
Wieshammer S, Dreyhaupt J. Dry powder inhalers: which factors determine the frequency of handling errors? Respiration. 2008;75:18–25.
Article
PubMedGoogle Scholar
-
Capstick T, Clifton I, Morgan J, Silcock J, Blenkinsopp A. Inhaler technique: an unmet need in patients with difficult asthma? Eur Respir J. 2013;42:A-4893.
Google Scholar
-
Nama S, Percival M, Harris M, Nolan-Neylan S, Sivakumaran P, Sriram K, Harland K. Evaluation of inhaler technique and medication adherence in COPD patients. Respirology. 2014;19:A-TP146.
Google Scholar
-
Vanderman AJ, Moss JM, Bailey JC, Melnyk SD, Brown JN. Inhaler misuse in an older adult population. Consult Pharm. 2015;30:92–100.
Article
PubMedGoogle Scholar
-
Pothirat C, Chaiwong W, Phetsuk N, Pisalthanapuna S, Chetsadaphan N, Choomuang W. Evaluating inhaler use technique in COPD patients. Int J Chron Obstruct Pulmon Dis. 2015;10:1291–8.
Article
CAS
PubMed
PubMed CentralGoogle Scholar
-
Madkour A, Galal I. Do Egyptian patients use their inhalers correctly? A checklist auditing for inhalation devices usage techniques. Egyptian J Chest Dis Tuberculosis. 2015;64:497–504.
Article
Google Scholar
-
Ozturk C, Aldag Y. Evaluation and importance of different types of inhaler device use in patients with chronic obstructive lung disease (COPD). Respirology. 2015;20(S3):A-471.
-
Chrystyn H, Price DB, Molimard M, Haughney J, Bosnic-Anticevich S, Lavorini F, Efthimiou J, Shan D, Sims E, Burden A. Comparison of serious inhaler technique errors made by device-naïve patients using three different dry powder inhalers: a randomised, crossover, open-label study. BMC Pulm Med. 2016;16:12.
Article
PubMed
PubMed Central
CASGoogle Scholar
-
Coelho ACC, Souza-Machado A, Leite M, Almeida P, Castro L, Cruz CS, Stelmach R, Cruz AA. Use of inhaler devices and asthma control in severe asthma patients at a referral center in the city of Salvador, Brazil. J Bras Pneumol. 2011;37:720–8.
Article
PubMedGoogle Scholar
-
Giraud V, Allaert FA, Roche N. Inhaler technique and asthma: Feasability and acceptability of training by pharmacists. Respir Med. 2011;105:1815–22.
Article
PubMedGoogle Scholar
-
Hagmolen of ten Have W, van de Berg NJ, Bindels PJ, van Aalderen WM, van der Palen J. Assessment of inhalation technique in children in general practice: increased risk of incorrect performance with new device. J Asthma. 2008;45:67–71.
Article
PubMedGoogle Scholar
-
Mehuys E, Boussery K, Adriaens E, van Bortel L, De Bolle L, van Tongelen I, Remon JP, Brusselle G. COPD management in primary care: an observational, community pharmacy-based study. Ann Pharmacother. 2010;44:257–66.
Article
PubMedGoogle Scholar
-
Molimard M, Gros VL. Impact of patient-related factors on asthma control. J Asthma. 2008;45:109–13.
Article
PubMedGoogle Scholar
-
Rajan S, Gogtay J. Ease-of-use, preference, confidence, and satisfaction with Revolizer, a novel dry powder inhaler, in an Indian population. Lung India. 2014;31:366–74.
Article
PubMed
PubMed CentralGoogle Scholar
-
Rootmensen G, Van Keimpema AR, Jansen HM, De Haan RJ. Predictors of incorrect inhalation technique in patients with asthma or COPD. Am J Respir Crit Care Med. 2010;181:A-3812.
Google Scholar
-
Schulte M, Osseiran K, Betz R, Wencker M, Brand P, Meyer T, Haidl P. Handling of and preferences for available dry powder inhaler systems by patients with asthma and COPD. J Aerosol Med Pulm Drug Deliv. 2008;21:321–8.
Article
CAS
PubMedGoogle Scholar
-
Van Der Palen J, Ginko T, Kroker A, Van Der Valk P, Goosens M, Padulles L, Seoane B, Rekeda L, Gil EG. Comparison of the preference, satisfaction, and critical errors made with Genuair and Handihaler in patients with COPD. Chest. 2012;142:A-717A.
Article
Google Scholar
-
Molimard M. How to achieve good compliance and adherence with inhalation therapy. Curr Med Res Opin. 2005;21:S33–7.
Article
PubMedGoogle Scholar
-
Westerik JA, Carter V, Chrystyn H, Burden A, Thompson SL, Ryan D, Gruffydd-Jones K, Haughney J, Roche N, Lavorini F, et al. Characteristics of patients making serious inhaler errors with a dry powder inhaler and association with asthma-related events in a primary care setting. J Asthma. 2016;53:321–9.
Article
PubMed
PubMed CentralGoogle Scholar
-
Chrystyn H, Bosnic-Anticevich S, Roche N, Molimard M, Haughney J, Lavorini F, Shan D, Sims E, Burden A, Ashton VL. Prevalence of serious post-training inhaler technique errors made by device-naïve patients using three different dry powder inhalers (DPIs). Eur Respir J. 2015;46:A-P3927.
Google Scholar
-
Thomas M, Van der Palen J, Chrystyn H, Sharma R, Imber V, Zhu C-Q, Barnes N. Inhaler errors and preference: a comparison of two multi-dose powder asthma inhalers. Respirology. 2015;20:A-573.
Article
Google Scholar
-
Li H, Chen Y, Zhang Z, Dong X, Zhang G, Zhang H. Handling of diskus dry powder inhaler in Chinese chronic obstructive pulmonary disease patients. J Aerosol Med Pulm Drug Deliv. 2014;27:219–27.
Article
PubMedGoogle Scholar
-
Melani AS, Canessa P, Coloretti I, Deangelis G, Detullio R, Del Donno M, Giacobbe R, Scarlato I, Serafini A, Barbato N, et al. Inhaler mishandling is very common in patients with chronic airflow obstruction and long-term home nebuliser use. Respir Med. 2012;106:668–76.
Article
PubMedGoogle Scholar
-
Capanoglu M, Dibek Misirlioglu E, Toyran M, Civelek E, Kocabas CN. Evaluation of inhaler technique, adherence to therapy and their effect on disease control among children with asthma using metered dose or dry powder inhalers. J Asthma. 2015;52:838–45.
Article
PubMed
CASGoogle Scholar
-
Pascual S, Feimer J, De Soyza A, Sauleda Roig J, Haughney J, Padulles L, Seoane B, Rekeda L, Ribera A, Chrystyn H. Preference, satisfaction and critical errors with Genuair and Breezhaler inhalers in patients with COPD: a randomised, cross-over, multicentre study. NPJ Prim Care Respir Med. 2015;25:15018.
Article
PubMed
PubMed CentralGoogle Scholar
-
Bryant L, Bang C, Chew C, Hee Baik S, Wiseman D. Adequacy of inhaler technique used by people with asthma or chronic obstructive pulmonary disease. JJ Prim Health Care. 2013;5:191–8.
Google Scholar
-
Dalcin PTR, Grutcki DM, Laporte PP, de Lima PB, Menegotto SM, Pereira RP. Factors related to the incorrect use of inhalers by asthma patients. J Bras Pneumol. 2014;40:13–20.
Article
PubMed CentralGoogle Scholar
-
Giraud V, Allaert FA, Magnan A. A prospective observational study of patient training in use of the autohaler inhaler device: the sirocco study. Eur Rev Med Pharmacol Sci. 2011;15:563–70.
CAS
PubMedGoogle Scholar
-
Harnett CM, Hunt EB, Bowen BR, O’Connell OJ, Edgeworth DM, Mitchell P, Eustace JA, Henry MT, Kennedy MP, Plant BJ, Murphy DM. A study to assess inhaler technique and its potential impact on asthma control in patients attending an asthma clinic. J Asthma. 2014;51:440–5.
Article
CAS
PubMedGoogle Scholar
-
Loh LC, Teng CL, Teh PN, Koh CN, Vijayasingham P, Thayaparan T. Metered-dose inhaler technique in asthmatic patients — a revisit of the Malaysian scene. Med J Malaysia. 2004;59:335–41.
CAS
PubMedGoogle Scholar
-
Chorao P, Pereira AM, Fonseca JA. Inhaler devices in asthma and COPD — an assessment of inhaler technique and patient preferences. Respir Med. 2014;108:968–75.
Article
PubMedGoogle Scholar
-
Hammerlein A, Muller U, Schulz M. Pharmacist-led intervention study to improve inhalation technique in asthma and COPD patients. J Eval Clin Pract. 2011;17:61–70.
Article
PubMedGoogle Scholar
-
Al-Hassan MI. Assessment of inhaler technique in patients attending a chest hospital in Riyadh City. Int J Pharmacol. 2009;5:232–5.
Article
Google Scholar
-
Komase Y, Asako A, Kobayashi A, Sharma R. Ease-of-use preference for the ELLIPTA dry powder inhaler over a commonly used single-dose capsule dry powder inhaler by inhalation device-naive Japanese volunteers aged 40 years or older. Int J COPD. 2014;9:1365–75.
Article
Google Scholar
-
Ozturk C, Kaya A, Bilgin C, Yucesoy L, Ikidag B, Demirel M, Baslilar S, Saylan B, Senol T, Aganoglu S, et al. Evaluation of inhaler technique and patient satisfaction with fixed-combination budesonide/formoterol dry-powder inhaler in chronic obstructive pulmonary disease (COPD): data on real-life clinical practice in Turkey. Tuberk Toraks. 2012;60:301–13.
Article
PubMedGoogle Scholar
-
Nolan-Neylan S, Harris M, Harland K, Sriram K. Evaluation of inhaler technique in hospitalised COPD patients. Respirology. 2015;20:A-P002.
Google Scholar
-
Lee SM, Chang YS, Kim CW, Kim TB, Kim SH, Kwon YE, Lee JM, Lee SK, Jeong JW, Park JW, et al. Skills in handling Turbuhaler, Diskus, and pressurized metered-dose inhaler in Korean asthmatic patients. Allergy Asthma Immunol Res. 2010;3:46–52.
Article
PubMed
PubMed CentralGoogle Scholar
-
Al-Jahdali H, Ahmed A, Al-Harbi A, Khan M, Baharoon S, Bin Salih S, Halwani R, Al-Muhsen S. Improper inhaler technique is associated with poor asthma control and frequent emergency department visits. Allergy Asthma Clin Immunol. 2013;9:8.
Article
PubMed
PubMed CentralGoogle Scholar
-
Maricoto T, Rodrigues LV, Teixeira G, Valente C, Andrade L, Saraiva A. Assessment of inhalation technique in clinical and functional control of asthma and chronic obstructive pulmonary disease. Acta Med Port. 2015;28:702–7.
Article
PubMedGoogle Scholar
-
Manriquez P, Acuna AM, Munoz L, Reyes A. Study of inhaler technique in asthma patients: differences between pediatric and adult patients. J Bras Pneumol. 2015;41:405–9.
Article
PubMed
PubMed CentralGoogle Scholar
-
Sriram KB, Percival M. Suboptimal inhaler medication adherence and incorrect technique are common among chronic obstructive pulmonary disease patients. Chron Respir Dis. 2015;13:13–22.
Article
PubMed
PubMed CentralGoogle Scholar
-
Buset EMN, Liaaen ED, Roth K, Blix HS. Inhalation technique in hospitalized asthma and COPD patients: should patients be regularly assessed before discharge? Int J Clin Pharm. 2015;37:A-16.
Google Scholar
-
Cayo-Quiñe A, Martínez-Vargas V, Bustamante-Voysest R, Piscoya A, Alberca Y: Incorrect use of metered-dose inhalers in adult patients at a hospital in Callao, Peru, 2014: cross-sectional study. Medwave 2014, 15:e6163-e6163.
-
Sangita P, Gharti KP, Laxman B. Assessment of inhalation techniques in COPD patients using metered-dose inhaler and Rotahaler at a tertiary care hospital in Nepal. Int Res J Pharm. 2015;6:288–93.
Article
Google Scholar
-
Villamil-Osorio M, Medina L, Pernett L, Restrepo SM, Nino G, Rodriguez-Martinez C. Assessment of inhalation technique and predictors of poor inhalation technique in a population of asthmatic children. J Aerosol Med Pulm Drug Deliv. 2015;191:A-3370.
Google Scholar
-
Udwadia ZZ, Kathar S, Shah HD, Pandey K, Rastogi S, Mullerpattan J. Who will teach the teachers: an analysis of the inhaler technique of Indian patients and health care providers. Am J Res Crit Care Med. 2013;187:A5026.
-
Turan P, Itil O, Turan M. Factors effecting inhaler technique in COPD. Am J Res Crit Care Med. 2014;189:A-6000.
-
Wu H, Thomas L, Bime C. An assessment of inhaler technique among patients with chronic obstructive airway diseases in a health professional shortage area. Am Philos Soc. 2013;187:A4208.
-
Baddar S, Jayakrishnan B, Al-Rawas OA. Asthma control: importance of compliance and inhaler technique assessments. J Asthma. 2014;51:429–34.
Article
PubMedGoogle Scholar
-
Sadowski C, Banh H, Cor K, Cave A. Inhaler device technique in community-dwelling older adults. Canadian Journal of. Hosp Pharm. 2013;66(4):269.
Google Scholar
-
Camilleri K, Balzan M, Bardon MP, Schembri E, Sullivan M, Mifsud S, Muscat D, Asciaq R, Montefort S. Predictors of good inhaler technique in asthma and COPD. Eur Respir J. 2015;46:A-P3928.
Google Scholar
-
Ganguly A, Das A, Roy A, Adhikari A, Banerjee J, Sen S. Study of proper use of inhalational devices by bronchial asthma or copd patients attending a tertiary care hospital. J Clin Diagn Res. 2014;8:HC04–7.
PubMed
PubMed CentralGoogle Scholar
-
Khassawneh BY, Al-Ali MK, Alzoubi KH, Batarseh MZ, Al-Safi SA, Sharara AM, Alnasr HM. Handling of inhaler devices in actual pulmonary practice: metered-dose inhaler versus dry powder inhalers. Respir Care. 2008;53:324–8.
PubMed
Google Scholar
-
Barthwal MS, Katoch CDS, Marwah V. Impact of optimal asthma education programme on asthma morbidity, inhalation technique and asthma knowledge. J Assoc Physicians India. 2009;57:574–9.
CAS
PubMedGoogle Scholar
-
Basheti IA, Armour CL, Bosnic-Anticevich SZ, Reddel HK. Evaluation of a novel educational strategy, including inhaler-based reminder labels, to improve asthma inhaler technique. Patient Educ Couns. 2008;72:26–33.
Article
PubMedGoogle Scholar
-
Burkhart PV, Rayens MK, Bowman RK. An evaluation of children’s metered-dose inhaler technique for asthma medications. Nurs Clin N Am. 2005;40:167–82.
Article
Google Scholar
-
Carpenter DM, Lee C, Blalock SJ, Weaver M, Reuland D, Coyne-Beasley T, Mooneyham R, Loughlin C, Geryk LL, Sleath BL. Using videos to teach children inhaler technique: a pilot randomized controlled trial. J Asthma. 2015;52:81–7.
Article
PubMedGoogle Scholar
-
Garcia-Cardenas V, Sabater-Hernandez D, Kenny P, Martinez-Martinez F, Faus MJ, Benrimoj SI. Effect of a pharmacist intervention on asthma control. A cluster randomised trial. Respir Med. 2013;107:1346–55.
Article
PubMedGoogle Scholar
-
Goris S, Tasci S, Elmali F. The effects of training on inhaler technique and quality of life in patients with COPD. J Aerosol Med Pulm Drug Deliv. 2013;26:336–44.
Article
PubMed
CASGoogle Scholar
-
Hesselink AE, Penninx BWJH, Van Der Windt DAWM, Van Duin BJ, De Vries P, Twisk JWR, Bouter LM, Van Eijk JTM. Effectiveness of an education programme by a general practice assistant for asthma and COPD patients: results from a randomised controlled trial. Patient Educ Couns. 2004;55:121–8.
Article
PubMedGoogle Scholar
-
Levy ML, Hardwell A, McKnight E, Holmes J. Asthma patients’ inability to use a pressurised metered-dose inhaler (pMDI) correctly correlates with poor asthma control as defined by the global initiative for asthma (GINA) strategy: a retrospective analysis. Prim Care Res J. 2013;22:406–11.
Google Scholar
-
Maazuddin M, Hazari MAH, Hasan A, Javeedullah M, Nasir Mohiuddin M, Baig MMA. Training in the use of inhalation devices and respiratory improvement in asthma and COPD patients: a before-after experimental study. Pharmanest. 2014;5:2314–20.
Google Scholar
-
Minai BA, Martin JE, Cohn RC. Results of a physician and respiratory therapist collaborative effort to improve long-term metered-dose inhaler technique in a pediatric asthma clinic. Respir Care. 2004;49:600–5.
PubMed
Google Scholar
-
Van Der Palen J, Eijsvogel MM, Kuipers BF, Schipper M, Vermue NA. Comparison of the Diskus inhaler and the Handihaler regarding preference and ease of use. J Aerosol Med. 2007;20:38–44.
Article
PubMedGoogle Scholar
-
Yildiz F, Erbagci A, Demirel YS, Akcali SD, Ekici A, Dursunoglu N, Ediger D, Erdinc M, Cemri SC, Kalyoncu AF, et al. Importance of inhaler device use status in the control of asthma in adults: the asthma inhaler treatment study. Respir Care. 2014;59:223–30.
Article
PubMedGoogle Scholar
-
Elgendy MO, Abdelrahim ME, Eldin RS. Potential benefit of repeated MDI inhalation technique counselling for patients with asthma. Eur J Hosp Pharm. 2015;22:318–22.
Article
Google Scholar
-
Grover C, Goel N, Armour C, Van Asperen P, Gaur S, Moles R, Saini B. Medication education program for Indian children with asthma: a feasibility study. Niger J Clin Pract. 2016;19:76–84.
Article
CAS
PubMedGoogle Scholar
-
Kuna P, Kupryś-Lipińska I, Dębowski T. Control of asthma in adults treated with beclomethasone and formoterol in extrafine particle formulation in a real-life setting in Poland: the CASPER noninterventional, observational trial. Pol Arch Med Wewn. 2015;125:731–40.
PubMed
Google Scholar
-
Plaza V, Peiró M, Torrejón M, Fletcher M, López-Viña A, Ignacio JM, Quintano JA, Bardagí S, Gich I. A repeated short educational intervention improves asthma control and quality of life. Eur Respir J. 2015;46:1298–307.
Article
CAS
PubMedGoogle Scholar
-
Bell D, Mansfield L, Lomax M, Dissanayake S. Patient handling study of fluticasone propionate/formoterol fumarate pressurized metered-dose inhaler. Respirology. 2014;19:A-O016.
Google Scholar
-
Kuprys-Lipinska I, Wiacek K, Przyrowski R, Kuna P. The educational program on the inhalation technique in a group of patients with asthma and COPD using Aerolizer — the effectiveness and the patients’ satisfaction. J Allergy Clin Immunol. 2011;1:A-443.
Google Scholar
-
Lin HL, Ng SP, Chen CH, Chien SY. Pharmacist-led educational interventions to improve inhalation technique in pediatric asthma patients. Pharmacoepidemiol Drug Saf. 2014;23:A-P414.
Google Scholar
-
Shetty F, Gupta R. Improved MDI inhaler technique observed in adult asthma patients with web based education. Eur Respir J. 2013;42:A-4959.
Google Scholar
-
Takemura M, Mitsui K, Ido M, Koyama M, Matsumoto M, Inoue D, Takamatsu K, Itotani R, Ishitoko M, Suzuki S. Clinical impact of a program to educate community pharmacists in providing proper inhalation technique for asthma patients. Eur Respir J. 2011;38:2845.
-
Maricoto T, Madanelo S, Rodrigues L, Teixeira G, Valente C, Andrade L, Saraiva A. Inhalation technique education and its impact in asthma and COPD. Eur Respir J. 2015;46:A-P5019.
Google Scholar
-
Fernandes L, Mesquita A. Improving asthma control with therapeutic education intervention. Eur Respir J. 2011;38:A-P4997.
Google Scholar
-
Barnestein-Fonseca P, Leiva-Fernández F, Vazquez-Alarcon R, Aguiar-Leiva V, Lobnig-Becerra M, Leiva-Fernández J. Can we improve the inhalation techniques in patients with COPD? Tiepoc study. Value Health. 2015;7:A-PRS10.
Google Scholar
-
Van Der Valk P, Goosens M, Groothuis-Oudshoorn K, Brusse-Keizer M, van der Palen J. Comparing the ease of use, preference and satisfaction of Accuhaler/Diskus and Elpenhaler in patients with asthma or chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187:A2336.
-
Prieto-Centurion V, Bracken NE, Jaffe HA, Hauser J, Norwick L, Krishnan JA, Zaidi F. Reducing avoidable readmissions following COPD exacerbations among US veterans: the importance of teaching appropriate use of respiratory inhalers. Am J Respir Crit Care Med. 2015;191:A6177.
-
Wiacek K, Kuna P, Kuprys-Lipinska I. The clinical effectiveness of the improvement of the inhalation technique in patients using aerolizer-2nd phase of the educational-observational program. American J Res Crit Care Med. 2012:185, A-5625.
-
Lee S-Y, Park H-W, Song W-J, Cho S-H. A multifaceted approach to reduce acute exacerbations in elderly asthmatics. Chest. 2015;148:A-11A.
Article
Google Scholar
-
Ammari W, Al-Hyari N, Obeidat N, Khater M, Sabouba A, Sanders M. Improving paediatrics’ pressurised metered dose inhaler technique and asthma control: inhaler verbal counselling vs. Trainhaler. Thorax. 2015;70:A-P100.
Article
Google Scholar
-
Ronk J, Alarcon L, Loughlin C. Implementing standardized metered-dose-inhaler (MDI) spacer technique checklist for pediatric asthma patients across University of North Carolina (UNC) Children’s hospital. Am J Respir Crit Care Med. 2012;185:A-3359.
Google Scholar
-
Al-Doghim I. Evaluation of inhalation technique of metered dose inhaler (MDI) and dry powder inhaler-Turbuhaler (DPI) among pediatric patients with asthma. J Appl Sci. 2007;9:53–66.
Google Scholar
-
Khan G, Badri P, Parbati T, Anita D, Atul A, Deepak P, Dipendra R, Himal B, Kabita G, Nirmala K. Intervention on inhalation technique of Rotahaler in patients with chronic obstructive pulmonary disease and asthma. Asian J Pharm Sci. 2016;11:81–2.
Article
Google Scholar
-
Alsomali H, Vines DL, Stein BD, EA B: Evaluating the health literacy and effectiveness of written dry powder inhaler instructions in patients diagnosed with chronic obstructive pulmonary disease. Am Assoc Res Care Open Forum 2015, 60:A-2303288.
-
Benjamin JA, Williams R, Bruce K, Jones O, Philips L. A 2 year programme to improve inhaler technique for adult patients with asthma and chronic obstructive pulmonary disease in a welsh university health board. Eur Respir J. 2015;46:A-P3929.
Google Scholar
-
Sulaiman I, MacHale E, Seheult J, D’Arcy S, Rapcan V, Mokoka M, Cushen B, Killane I, Franciosi A, Sahadevan A. Feedback on adherence and inhaler technique using the Inca device: a randomised control trial in severe asthma. Am J Respir Crit Care Med. 2016;193:A-1714.
Google Scholar
-
Thomas M, Van Der Palen J, Chrystyn H, Zhu C, Ghatta S, Svedsater H. Time to achieve correct inhaler use and inhaler preference: a comparison of Ellipta® with three inhaler devices in patients with asthma. Am J Respir Crit Care Med. 2016;193:A-1739.
Google Scholar
-
Van Der Palen J, Thomas M, Chrystyn H, Sharma R, Imber V, Zhu C-Q, Svedsater H. Training and time to achieve correct inhaler use: a comparison between inhalers in patients with COPD. In: AJRCCM conference. San Francisco, CA, US: American Thoracic Society; 2016. p. A-6812.
Google Scholar
-
Juniper EF, O’Byrne PM, Guyatt GH, Ferrie PJ, King DR. Development and validation of a questionnaire to measure asthma control. Eur Respir J. 1999;14:902–7.
Article
CAS
PubMedGoogle Scholar
-
Nathan RA, Sorkness CA, Kosinski M, Schatz M, Li JT, Marcus P, Murray JJ, Pendergraft TB. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004;113:59–65.
Article
PubMedGoogle Scholar
-
Azevedo P, Correia de Sousa J, Bousquet J, Bugalho-Almeida A, Del Giacco SR, Demoly P, Haahtela T, Jacinto T, Garcia-Larsen V, van der Molen T, et al. Control of allergic rhinitis and asthma test (CARAT): dissemination and applications in primary care. Prim Care Res J. 2013;22:112–6.
Google Scholar
-
Skinner EA, Diette GB, Algatt-Bergstrom PJ, Nguyen TT, Clark RD, Markson LE, AW W. The asthma therapy assessment questionnaire (ATAQ) for children and adolescents. Dis Manag. 2004;7:305–13.
Article
PubMedGoogle Scholar
-
Murphy KR, Zeiger RS, Kosinski M, Chipps B, Mellon M, Schatz M, Lampl K, Hanlon JT, Ramachandran S. Test for respiratory and asthma control in kids (TRACK): a caregiver-completed questionnaire for preschool-aged children. J Allergy Clin Immunol. 2009;123:833–9. e839
Article
PubMedGoogle Scholar
-
Groot EP, Kreggemeijer WJ, Brand PL. Getting the basics right resolves most cases of uncontrolled and problematic asthma. Acta Paediatr. 2015;104:916–21.
Article
PubMedGoogle Scholar
-
Zaidi S, Williams J, Monaghan T, Burhan H, Main N. Inhaler Technique: Does Poor Technique Mean More Admissions? Am J Respir Crit Care Med. 2012;185:A-3333.
Google Scholar
-
Roggeri A, Micheletto C, Boarino S, Inzillo V, Roggeri DP. Potential economic impact of inhalation errors due to device switch in patients with chronic obstructive pulmonary disease and asthma. Value Health. 2015;18:A-PMD147.
Google Scholar
-
Roggeri A, Micheletto C, Roggeri DP. Inhalation errors due to device switch in patients with chronic obstructive pulmonary disease and asthma: critical health and economic issues. Int J Chron Obstruct Pulmon Dis. 2016;11:597–602.
Article
PubMed
PubMed CentralGoogle Scholar
-
Bijos P, Kaczynski J, Torvinen S, Lenarczyk E, Wrona W, Plich A, Lewis A, Blackney M. Clinical and economic burden of asthma and chronic obstructive pulmonary disease (COPD) in Poland: estimated impact of poor inhalation technique with inhaled corticosteroid and long-acting beta agonist fixed-dose combinations. Value Health. 2015;18:A-PRS34.
Article
Google Scholar
-
Torvinen S, Nicolai J, Pulimeno S, di Nola L, Bruno G, Colombo G, Di Matteo S, Valentino M, Lewis A, Blackney M. The budget impact of Duoresp® Spiromax® compared with commonly prescribed dry powder inhalers for the management of asthma and chronic obstructive pulmonary disease in Italy: estimated impact of inhalation technique. Value Health. 2015;18:A-PRS16.
Google Scholar
-
Lewis A, Blackney M, Torvinen S, Plich A. Clinical and economic burden of asthma and chronic obstructive pulmonary disease in the UK: impact of critical inhaler errors with inhaled corticosteroid + long-acting beta agonist fixed-dose combinations. Value Health. 2014;17:A-PRS30.
Article
Google Scholar
-
Lewis A, Blackney M, Garcia BL, Sánchez-de la Rosa R, Torvinen S, Plich A. The potential for improved inhalation technique with Duoresp® Spiromax®(budesonide+formoterol fumarate dihydrate) compared with commonly prescribed dry powder inhalers for the management of asthma and chronic obstructive pulmonary disease in Spain: estimated impact on number and cost of unscheduled healthcare events. Value Health. 2015;18:A-PMD37.
Google Scholar
-
Lewis A, Blackney M, Torvinen S, Lindqvist F, Safioti G, Grundstrom J, Polyzoi M, Plich A. The potential societal cost benefits of improved inhalation technique with Duoresp Spiromax (budesonide + formoterol fumarate dihydrate) compared with Symbicort Turbuhaler for the management of asthma and chronic obstructive pulmonary disease in sweden. Value Health. 2014;17:A-PRS62.
Article
Google Scholar
-
Lewis A, Blackney M, Torvinen S, Holmes J, Osborne M, Dale J, Chandler S, Plich A. The budget impact of Duoresp Spiromax (budesonide + formoterol fumarate dihydrate) compared with Symbicort Turbohaler for the management of asthma and chronic obstructive pulmonary disease in the United Kingdom: impact on health care costs and inhalation technique. Value Health. 2014;17:A-PRS19.
Article
Google Scholar
-
Estrada J, Restrepo A, Serna J, Herrera R, Arrieta J, Segura A. Impact of a pharmacotherapeutic follow-up program on the cost-month-patient, stratified by risk-pharmacological type. Value Health. 2015;18:A-PRS14.
Google Scholar
-
Basheti I, Bosnic-Anticevich S, Armour C, Reddel H. Checklists for powder inhaler technique: a review and recommendations. Respir Care. 2014;59:1140–54.
Article
PubMedGoogle Scholar
-
Basheti IA, Reddel HK, Armour CL, Bosnic-Anticevich SZ. Improved asthma outcomes with a simple inhaler technique intervention by community pharmacists. J Allergy Clin Immunol. 2007;119:1537–8.
Article
PubMedGoogle Scholar
-
Sulaiman I, Seheult J, Sadasivuni N, Cushen B, Mokoka M, Costello R. Inhaler technique errors have an impact on drug delivery. Am J Respir Crit Care Med. 2016;193:A-1715.
Google Scholar
-
Molimard M, Raherison C, Lignot S, Balestra A, Lamarque S, Chartier A, Droz-Perroteau C, Lassalle R, Moore N, Girodet P-O. Chronic obstructive pulmonary disease exacerbation and inhaler device handling: real-life assessment of 2935 patients. Eur Respir J. 2016;49
-
Price DB, Roman-Rodriguez M, McQueen RB, Bosnic-Anticevich S, Carter V, Gruffydd-Jones K, Haughney J, Henrichsen S, Hutton C, Infantino A, et al. Inhaler errors in the CRITIKAL study: type, frequency, and association with asthma outcomes. J Allergy Clin Immunol Pract. 2017;5:1071–1081.e1079.
Article
PubMedGoogle Scholar
-
Williams SA, Wagner S, Kannan H, Bolge SC. The association between asthma control and health care utilization, work productivity loss and health-related quality of life. J Occup Environ Med. 2009;51:780–5.
Article
PubMedGoogle Scholar
-
Vervloet D, Williams A, Lloyd A, Clark T. Costs of managing asthma as defined by a derived asthma control TestTM score in seven European countries. Eur Respir Rev. 2006;15:17–23.
Article
Google Scholar
-
Szende A, Svensson K, Ståhl E, Meszaros A, Berta GY. Psychometric and utility-based measures of health status of asthmatic patients with different disease control level. PharmacoEconomics. 2004;22:537–47.
Article
PubMedGoogle Scholar
-
Doz M, Chouaid C, Com-Ruelle L, Calvo E, Brosa M, Robert J, Decuypere L, Pribil C, Huerta A, Detournay B. The association between asthma control, health care costs, and quality of life in France and Spain. BMC Pulm Med. 2013;13:15.
Article
PubMed
PubMed CentralGoogle Scholar
-
Demoly P, Annunziata K, Gubba E, Adamek L. Repeated cross-sectional survey of patient-reported asthma control in Europe in the past 5 years. Eur Respir Rev. 2012;21:66–74.
Article
CAS
PubMedGoogle Scholar
-
Jha A, Heron L, Marshall J, Dunlop W. Device handling errors and the impact on quality of life and health care resource use in asthmatic patients. Value Health. 2014;17:A-PRS64.
Google Scholar
-
Scichilone N, Benfante A, Bocchino M, Braido F, Paggiaro P, Papi A, Santus P, Sanduzzi A. Which factors affect the choice of the inhaler in chronic obstructive respiratory diseases? Pulm Pharmacol Ther. 2015;31:63–7.
Article
CAS
PubMedGoogle Scholar
-
Lavorini F, Mannini C, Chellini E, Fontana GA. Optimising inhaled pharmacotherapy for elderly patients with chronic obstructive pulmonary disease: the importance of delivery devices. Drugs Aging. 2016;33:461–73.
Article
CAS
PubMedGoogle Scholar
-
Perez L, Morales K, Huang J, Ndicu G, Han X, Klusaritz H, Localio A, Apter AJ. Aspects of asthma self-management: inhaler technique, ability to access (navigate) health care, and inhaled steroid knowledge are correlated. Am J Res Crit Care Med. 2016;193:A6426.
-
Kiser K, Jonas D, Warner Z, Scanlon K, Shilliday BB, DeWalt DA. A randomized controlled trial of a literacy-sensitive self-management intervention for chronic obstructive pulmonary disease patients. The. J Gen Intern Med. 2012;27:190–5.
Article
PubMedGoogle Scholar
-
Paasche-Orlow MK, Riekert KA, Bilderback A, Chanmugam A, Hill P, Rand CS, Brancati FL, Krishnan JA. Tailored education may reduce health literacy disparities in asthma self-management. Am J Respir Crit Care Med. 2005;172:980–6.
Article
PubMed
PubMed CentralGoogle Scholar
-
Al Zabadi H, El Sharif N. Factors associated with frequent emergency room attendance by asthma patients in Palestine. Int J Tuberc Lung Dis. 2007;11:920–7.
CAS
PubMedGoogle Scholar
-
Azouz W, Chetcuti P, Hosker H, Saralaya D, Chrystyn H. Objective measurement of inhalation profiles in patients using metered dose inhalers (MDIs). Eur Respir J. 2011;38:A-838.
Google Scholar
-
Baddar S, Al-Rawas O. What is missing in the asthma control test? The relationship between compliance, inhaler technique and level of control. Eur Respir J. 2012;40:A-P513.
Article
Google Scholar
-
Bilal M, Ahmed A, Shah AR, Mirza HA, Anwar AK, Zaidi SBH. Prevalence of the correct technique of using an inhaler among asthmatic patients reporting in tertiary care hospitals of Rawalpindi, Pakistan. J Allergy Clin Immunol. 2012;1:A-159.
Google Scholar
-
Caliskaner Z, Ozturk C, Pekcan S, Yilmaz O, Ozturk S, Ceylan E, Can C, Sener O, Turay U, Ersoy R. The «extreme» errors in inhaler device use: data from the INTEDA-1 study. In: Allergy; 2011. p. 369–70.
Google Scholar
-
Chrystyn H, Pascual S, Feimer J, De Soyza A, Sauleda Roig J, Haughney J, Padulles L, Seoane B, Rekeda L, Ribera A. Preference, satisfaction and critical errors with Genuair and Breezhaler in patients with COPD. Eur Respir J. 2014;44:A-P928.
Google Scholar
-
Deering B, MacCormack N, Kerrigan K, D’Arcy S, Costello RW. Adherence to inhalers after discharge from hospital following an exacerbation of COPD. Ir J Med Sci. 2013;182:S458.
Google Scholar
-
Hass C, Engdahl K, Albert W, Setyawan J, Mateo N. Patient preferences and perceived ease of use in inhaler features: Genuair vs other inhalers. Chest. 2010;138:A-484.
Article
Google Scholar
-
Herscher M, Ray M, Busse PJ, Wolf MS, Wisnivesky JP, Federman A. Characteristics and outcomes of older adults with early versus late onset asthma. Am J Respir Crit Care Med. 2014;189:A-1359.
Article
CASGoogle Scholar
-
Leiva-Fernandez F, Leiva-Fernandez J, Porcel-Martin C, Prados-Torres D, Garcia-Ruiz AJ, Barnestein-Fonseca P. How do patients with chronic obstructive pulmonary disease (COPD) use their inhalers? Common mistakes. Tecepoc study. Value Health. 2013;16:A-PRS45.
Google Scholar
-
Mazankova D, Mendelova I, Saloun J. Identification of error rate in using inhalation devices by asthmatic patients. Int J Clin Pharm. 2013;35(6):1279–80.
Google Scholar
-
Muhammad I, Haque AS, Muhammad N, Khan JA. Real life perspective in outpatient asthma treatment at a tertiary care center of Pakistan. Respirology. 2009;14:A-PD 10-09.
Google Scholar
-
Santos JC, Silveira BF, Rizzatti F. Knowledge of and technique for using inhalation devices among asthma and COPD patients. Am J Res Crit Care Med. 2014;A-4656
-
Souza M, Meneghini A, Ferraz E, Vianna E, Borges M. Knowledge of and technique for using inhalation devices among asthma patients and COPD patients. J Bras Pneumol. 2009;35:824–31.
Article
PubMedGoogle Scholar
-
Tarsin W, Alshamli I, Soussi M. Preference of the inhaler device and assessment of the technique among the asthmatic and COPD patients. Eur Respir J. 2011;38:A-3981.
Google Scholar
-
Williams J, Mault S, Garner N, Burhan H, Zaidi S. Breaking down bad inhaler technique: device specific advice. Am J Respir Crit Care Med. 2012;185:A-3332.
Google Scholar
Download references
Acknowledgements
We would like to thank Alison Saunders, Iván Viejo Viejo and Rebecca Forster for their support in quality checking and co-ordinating this manuscript and Robin Wyn for editorial assistance.
Funding
Funding was provided by Mundipharma International Ltd. to Adelphi Values Ltd. to support this research and the writing of the manuscript. No financial payment was provided to the individual authors of the review.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Trademark
® DISKHALER, DISKUS and ROTAHALER are registered trademarks of Glaxo Group Limited.
® ACCUHALER and EVOHALER are registered trademarks (in the European Union) of Glaxo Group Limited.
® REVOLIZER is a registered trade mark (in the United States) of Cipla Limited.
® AUTOHALER is a registered trade mark of 3 M Company.
® STARHALER is a registered trade mark (in India) of Sun Pharma Laboratories Limited.
® TURBUHALER is a registered trade mark (in the European Union) of AstraZeneca AB.
® HANDIHALER and HandiHaler are registered trademarks of Boehringer Ingelheim Pharma GmbH & Co. KG.
® AEROLIZER is a registered trade mark of Novartis AG.
® GENUAIR is a registered trade mark of AstraZeneca AB.
® BREEZHALER is a registered trade mark (in the European Union) of Novartis AG.
® ELPENHALER is a registered trade mark of Elpen Pharmaceutical Co. Inc.
® CYCLOHALER is a registered trade mark (in the European Union) of Pharmachemie B.V.
® EASI-BREATHE is a registered trade mark (in the European Union) of Norton Healthcare Limited.
® PULVINAL is a registered trade mark (in the European Union) of Chiesi Farmaceutici S.p.A.
® PULMOJET is a registered trade mark (in the European Union) of Sanofi S.A.
Author information
Authors and Affiliations
-
Airway Disease, NHLI, Imperial College London & Royal Brompton Hospital, Dovehouse Street, London, SW3 6LY, UK
Omar Sharif Usmani
-
Department of Experimental and Clinical Medicine, Careggi University Hospital, Florence, Italy
Federico Lavorini
-
Mundipharma International Limited, Cambridge Science Park, Cambridge, CB4 0AB, UK
Jonathan Marshall & William Christopher Nigel Dunlop
-
Adelphi Values, Adelphi Mill, Macclesfield, Cheshire, SK10 5JB, UK
Louise Heron & Emily Farrington
-
Radboud University Medical Center, Nijmegen, Netherlands
Richard Dekhuijzen
Authors
- Omar Sharif Usmani
You can also search for this author in
PubMed Google Scholar - Federico Lavorini
You can also search for this author in
PubMed Google Scholar - Jonathan Marshall
You can also search for this author in
PubMed Google Scholar - William Christopher Nigel Dunlop
You can also search for this author in
PubMed Google Scholar - Louise Heron
You can also search for this author in
PubMed Google Scholar - Emily Farrington
You can also search for this author in
PubMed Google Scholar - Richard Dekhuijzen
You can also search for this author in
PubMed Google Scholar
Contributions
All authors have contributed equally to the analysis, review, writing and finalisation of this manuscript. All authors have read and approved the final manuscript.
Corresponding author
Correspondence to
Omar Sharif Usmani.
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
In the last 5 years, Omar S. Usmani and/or his department received research grants, unrestricted educational grants, and/or fees for lectures and advisory board meetings from Aerocrine, Astra Zeneca, Boehringer Ingelheim, Chiesi, Cipla, Edmond Pharma, GlaxoSmithKline, Napp, Mundipharma International, Prosonix, Sandoz, Takeda, Zentiva.
In the last 5 years, Federico Lavorini received fees for lectures and advisory board meetings from Astra Zeneca, Boehringer Ingelheim, Chiesi, Cipla, Menarini International, TEVA, Zentiva.
In the last 3 years, Richard Dekhuijzen and/or his department received research grants, unrestricted educational grants, and/or fees for lectures and advisory board meetings from AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Mundipharma International, Novartis, Takeda and Teva.
William Dunlop and Jonathan Marshall are employees of Mundipharma International Ltd., United Kingdom.
Emily Farrington and Louise Heron are employees of Adelphi Values Ltd., UK. Adelphi Values Ltd. received funding from Mundipharma International Ltd. to support this research.
The authors do not report any conflict of interest with regards to the contents of this study other than those stated.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Additional file
Additional file 1:
One supplementary file is associated with this manuscript: “Online Resource – Critical handling errors in asthma and COPD: A systematic review of impact on health outcomes”. This contains: search strategies and details of the analysis conducted within this literature review (Table S1); a breakdown of grouped critical errors described in the literature for different inhaler device types (Table S2); summaries of pre-existing known publications that show associations between poor disease control, economic burden and poor QoL (Table S3); definitions of a ‘critical’ error provided by studies captured within the literature review (Table S4). This file is named: “Critical handling errors data supplement update v8_0”. (DOCX 588 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Reprints and Permissions
About this article
Cite this article
Usmani, O.S., Lavorini, F., Marshall, J. et al. Critical inhaler errors in asthma and COPD: a systematic review of impact on health outcomes.
Respir Res 19, 10 (2018). https://doi.org/10.1186/s12931-017-0710-y
Download citation
-
Received: 07 September 2017
-
Accepted: 21 December 2017
-
Published: 16 January 2018
-
DOI: https://doi.org/10.1186/s12931-017-0710-y
Keywords
- Obstructive lung diseases
- Adherence
- Errors
- Aerosols
- Inhalers
Ингаляция – эффективная процедура при заболеваниях дыхательных путей. Но иногда ингаляции усложняют ситуацию, и причина этому − неправильное применение прибора. Расскажем, какие ошибки при использовании небулайзеров нельзя допускать.
Семь ошибок при использовании небулайзера
- Самолечение
Выбор лекарственного препарата, длительности и кратности проведения процедур зависит от вида и тяжести заболевания. А диагностика и назначение лечения – это прерогатива врача.
- Использование масляных растворов
Капельки масла оседают на бронхах, нарушают газообмен и могут привести к опасным последствиям. Устройство же приходит в негодность и не подлежит ремонту.
Для проведения ингаляций можно использовать только специальные лекарства, предназначенные для небулайзерной терапии.
- Использование небулайзера сразу после другого члена семьи
Съемные элементы небулайзера следует обрабатывать после каждой процедуры в соответствии с инструкцией к прибору. Это исключает перекрестные инфекции, если небулайзером пользуются несколько людей.
- Несоблюдение времени и кратности выполнения ингаляций
Частота и время проведения процедур подбираются врачом в зависимости от вида и сложности заболевания.
- Отмена процедуры при повышенной температуре тела
Если состояние пациента удовлетворительное и иное не предписано врачом, ингаляции с помощью небулайзера можно делать и при повышенной температуре тела.
Гипертермия является противопоказанием для паровых ингаляций, но небулайзеры работают по другому принципу.
- Проведение ингаляций для лечения заболеваний, при которых небулайзерная терапия неэффективна
В небулайзере лекарственный раствор рассеивается до мелкого тумана с размером частиц 1−5 мкм. Аэрозоль оседает в средних и нижних отделах дыхательных путей. Процедуры помогают при трахеите, бронхите, бронхиальной астме и пневмонии. При фарингите и рините ингаляции будут неэффективны.
- Применение формированного дыхания
Дыхание во время ингаляции должно быть обычным, нефорсированным. Частое глубокое дыхание приводит к гипервентиляции легких и может вызвать головокружение.
Условия эффективности ингаляционной терапии
И.Э. Степанян
В статье рассматриваются особенности и сравнительная эффективность различных ингаляционных устройств. Особое внимание уделяется ошибкам при использовании дозированных аэрозольных ингаляторов и дозированных порошковых ингаляторов, а также особенностям экстрамелкодисперсных аэрозолей.
Ключевые слова: ингаляционные устройства, бронхиальная астма, хроническая обструктивная болезнь легких, дозированные аэрозольные ингаляторы, дозированные порошковые ингаляторы, экстрамелкодисперсные аэрозоли, легочная депозиция, ошибки при ингаляции, формотерол.
Ингаляционный путь введения лекарств широко применяется в лечении пациентов с заболеваниями органов дыхания: бронхиальной астмой, хронической обструк-тивной болезнью легких, муковисцидозом, бронхоэкта-тической болезнью, острым и хроническим бронхитом, артериальной легочной гипертензией. Прямая доставка препаратов к месту их действия в дыхательных путях позволяет добиться требуемого результата с использованием малых доз действующих веществ и минимизировать системные эффекты. Среди препаратов, применяемых ингаляционно, — бронхорасширяющие средства разных фармакологических групп, глюкокортикостероиды (ГКС), муколитики, антибиотики, антисептики, противогрибковые средства и др.
Виды ингаляционных устройств
За последние полвека было создано множество ингаляционных лекарственных препаратов и устройств для их доставки. Всё разнообразие ингаляционных устройств можно подразделить на следующие группы:
• дозированные аэрозольные ингаляторы (ДАИ), в том числе применяемые со спейсерами и клапанными аэрозольными камерами;
• ДАИ, активируемые вдохом;
• дозированные порошковые ингаляторы (ДПИ);
• небулайзеры;
• ингаляторы «мягкого» аэрозоля (soft mist inhalers).
Каждая группа устройств обладает определенными преимуществами и недостатками. В целом эффективность ингаляционной терапии определяется легочной депозици-ей вдыхаемых частиц, которая зависит от их размера и правильности выполнения дыхательных маневров пациентом. Нарушение проходимости дыхательных путей и турбулентность вдыхаемого воздушного потока в местах деления бронхов препятствуют проникновению частиц лекарств в периферические дыхательные пути.
Бурное развитие техники для ингаляционной терапии породило проблему выбора оптимального ингалятора для применения у той или иной категории пациентов. В 2011 г. Европейское респираторное общество опубликовало рекомендации по ингаляционной терапии в пульмонологической практике [1]. В этих рекомендациях сделан акцент на необходимости соблюдения пациентами правильной техники ингаляции и контроля со стороны врача за правильно-
Игорь Эмильевич Степанян — профессор, вед. науч. сотр. отдела дифференциальной диагностики туберкулеза легких и экстракорпоральных методов лечения Центрального НИИ туберкулеза РАМН, Москва.
стью пользования ингаляционными устройствами для достижения оптимального эффекта ингаляционной терапии. На практике эти правила довольно часто не соблюдаются. Так, было установлено, что, по крайней мере, одну ошибку в технике ингаляции допускают 76% пациентов, пользующихся ДАИ, и 49-54% больных, применяющих ДАИ, активируемые вдохом; от 4 до 94% пациентов неправильно пользуются ДПИ, а 25% никогда не обучались правильной технике ингаляции [2, 3].
Ошибки при использовании ДАИ и ДПИ
На протяжении многих лет основной проблемой при пользовании ДАИ остается координация вдоха с активацией ингалятора [4].
Факторами, достоверно повышающими риск критических ошибок при ингаляции с помощью ДАИ и ДПИ, являются:
Таблица 1. Ошибки пациентов при использовании ДАИ
Правила ингаляции Частота ошибок, %
Удалить защитный колпачок 0,15*
Встряхнуть ингалятор (в случае суспензии) 37
Произвести полный выдох перед активацией ингалятора 50
Держать ингалятор вертикально донышком вверх 9
Разместить загубник между губами, поверх языка, не перекрывая просвет 0,7*
Выполнить только одну активацию ингалятора во время вдоха 19
Выполнить активацию ингалятора в начале вдоха 18 — во второй половине вдоха, 5* — после окончания вдоха
Вдыхать глубоко и медленно (не прерывать вдох сразу после активации ингалятора) 10* — прерывание вдоха, 52 — форсированный вдох
Вдыхать через рот (не через нос) 2*
Задержать дыхание на 10 с на высоте вдоха 53
* Критические ошибки.
с
Таблица 2. Ошибки пациентов при использовании ДПИ
Правила ингаляции V Технические ошибки, % от числа всех пациентов
Аэролайзер/ХандиХалер Мультидиск Турбухалер
Удалить/повернуть крышку* 0 0,65 0
Вставить капсулу* 9 Неприменимо Неприменимо
Проколоть капсулу* 3 Неприменимо Неприменимо
Правильно загрузить дозу* Неприменимо 7,3 14
Держать ингалятор вертикально Неприменимо Неприменимо 23
Произвести полный выдох (не в ингалятор) 19 22 14
Разместить загубник между губами* 5 5 4
Вдыхать глубоко (не прерывать вдох сразу после активации ингалятора) 26 29 22
Вдыхать быстро (форсированный вдох)* 24 28 22
Вдыхать через рот (не через нос)* 2 1 0
Задержать дыхание на высоте вдоха 25 32 28
Выдохнуть не через загубник ингалятора 19 21 11
Проверить, что капсула не содержит остатков порошка 30 Неприменимо Неприменимо
* Критические ошибки.
• пожилои или детскии возраст;
• отсутствие инструктажа со стороны врача;
• деменция;
• низкий уровень образования;
• использование больным ингаляторов разных типов.
Неправильное пользование ингаляторами приводит к неполному контролю заболевания, более частому возникновению потребности в назначении пероральных ГКС и антибиотиков, увеличивает риск госпитализации [5, 6].
В табл. 1 и 2 суммированы ошибки, допускаемые пациентами при пользовании ДАИ и ДПИ, по данным А^. Ме!ап1 е! а!. [5]. Это многоцентровое наблюдательное исследование было проведено у 1664 больных хронической обструк-тивной болезнью легких и бронхиальной астмой, имеющих опыт использования ингаляторов (оценка проводилась с тем устройством, которым пользуется конкретный пациент). Критическими считались ошибки, которые существенно снижают легочную депозицию препарата. Результаты исследования свидетельствуют о том, что при исполь-
5 г
II
ill I з о
Ct £ ГО
о. 1 m ™
я I
2 —
1 —
0,8
Формотерол ДАИ (Атимос)
Формотерол ДПИ (Аэролайзер)
Рис. 1. Средний аэродинамический диаметр частиц аэрозоля формотерола, образуемого ДАИ и ДПИ.
зовании аэрозольных ингаляторов критические ошибки встречаются достоверно реже (18%), чем в случае порошковых ингаляторов (от 35 до 44% для различных устройств).
Критические ошибки пациентов сводят на нет ожидаемый эффект от ингаляционной терапии, поэтому рекомендации при каждом визите пациента проверять правильность соблюдения техники ингаляций, содержащиеся в руководствах GINA (Global Initiative for Asthma) и GOLD (Global Initiative for Chronic Obstructive Lung Disease), очень актуальны. Перед тем как назначить новый ингалятор, врач должен также оценить способность пациента правильно освоить технику пользования новым устройством.
Новые технологии производства ДАИ
В связи с вышеизложенным разработка новых препаратов и устройств для ингаляционной терапии направлена на упрощение ингаляционной техники и уменьшение вероятности ошибок, снижающих эффективность лечения. Одним из подходов к решению данной проблемы стала технология Модулит, которая была разработана компанией Chiesi для использования в бесфреоновых ДАИ. Технология Модулит, включающая добавление в лекарственную форму дополнительных компонентов и изменение геометрии устья актуа-тора, позволяет формировать аэрозольное облако с частицами заданного размера. Помимо возможности создавать экстрамелкодисперсные аэрозоли (с частицами размером менее 2 мкм) это приводит к снижению скорости аэрозоля и значительному увеличению времени «жизни» облачка аэрозоля (с 0,18 до 1,16 с).
Преимуществами технологии Модулит являются:
• возможность получать аэрозоль с частицами требуемого размера;
• уменьшение скорости струи аэрозоля;
• более продолжительное время жизни облачка аэрозоля;
• упрощение координации вдоха и нажатия на баллончик;
• уменьшение депозиции препарата в верхних дыхательных путях.
Л
с АТИМОС
i^
формотерол 12 м кг/доз«; 120 доз
АТИМОС (экстрамелкодисперсный формотерол) -беЗОШИбОЧНЫЙ Выбор для лечения пациентов
с любой категорией ХОБЛ1:
А: в монотерапии
В: в монотерапии (или в комбинации с тиотропием) С: в комбинации с ИГКС* (или с тиотропием) Р: в комбинации с ИГКС (или/и с тиотропием)
* АТИМос М<
Дэро.
ЗО/ТЬ
«агв & 5с
¿ » 1
®°Pmi
‘°герол
Входит в ЖНВЛП2 и лло3
* Ингаляционные глюкокортоюхлероцды.
1 Согласно QOLD 2011 формотерол может быть использован у всех категорий болы-ых ХОБЛ. Global Initiative for Coronta Obstructiva Lung Dlsease. Global Strategy 1or the Diagnosis, Management, and Prévention of Chranic Obstiuctive Pulmonaiy Disease. Revised 2011И www.goldcopd.org
2 Формотерол, аэрозоль для ингаляций дозированный, включен в перечень ЖНВЛП (Распоряжение Правительства Российской Федерации or 7 декабря 2011 г, Na 2199-р}
3 Приказ Минадравсоцразвитга России № 1340н от 10.11.2011 г. (Per. в MnnocreN 22368 от 23.11.2011 г.): обновленный Перечень лекарственных препаратов, вт.ч. перечень ЛП, назначаемых по решению врачебной комиссии ЛПУ, обеспечение изгорьми осуществляется в соответствии со стандартами медицинской помощи по рецептам врача (фельдшера) при оказании государственной социальной помощи в виде набора социальных услуг
ПЕРЕД ПРИМЕНЕНИЕМ НЕОБХОДИМО ОЗНАКОМИТЬСЯ С ИНСТРУКЦИЕЙ
С Chiesi
iНе можете найти то, что вам нужно? Попробуйте сервис подбора литературы.
ООО «Кьези Фармасьютикалс»
Тел.: (495) 967-12-12, факс: (495) 967-12-11 www.chiesi.ru
Рис. 2. Легочная депозиция формотерола у одного и того же пациента после ингаляции Атимоса (а) и ДПИ формотерола (б) (сцинтиграфия после ингаляции препарата с радиоизотопной меткой).
œ
и
а.
m га
16 14 12 10 8 6 4 2 0
12,2
4,8
5,5
2,7
_1_
_1_
_1_
_1_
7,4
_1_
70 60 50 40 30 20 Скорость вдоха, л/мин
10
Рис. 3. Зависимость размера частиц аэрозоля от скорости инспираторного потока при ингаляции формотерола через порошковый ингалятор Турбухалер.
Технология Модулит была использована при создании ряда ДАИ, как с обычным размером частиц (Кленил Джет -ДАИ с компактным спейсером, содержащий беклометазо-на дипропионат), так и экстрамелкодисперсных — Фостер (беклометазона дипропионат + формотерол) и Атимос (формотерол).
Рассмотрим особенности экстрамелкодисперсных ДАИ на примере Атимоса. Атимос образует экстрамелкодисперсный аэрозоль с размером частиц менее 1 мкм по сравнению с 3,5 мкм у порошковых ингаляторов формоте-рола, что позволяет ему хорошо проникать в малые дыхательные пути (рис. 1) [7, 8].
Благодаря малому размеру частиц и ингаляционному устройству (ДАИ) Атимос обеспечивает более высокую
легочную депозицию по сравнению с ДПИ формотерола (рис. 2) [7, 9].
Следует учитывать, что размер частиц аэрозоля, образуемого порошковым ингалятором, увеличивается по мере ослабления усилия на вдохе (нарастания обструкции), что ухудшает легочную депозицию из ДПИ (рис. 3) [10].
Результаты рандомизированного двойного слепого перекрестного исследования сравнительной эффективности разовой дозы формотерола в ДАИ (Атимос), формотерола в ДПИ (Аэролайзер) и плацебо (ДАИ или Аэролайзер) у пациентов со среднетяжелой и тяжелой бронхиальной астмой показали, что за 12-часовой период наблюдения Атимос обеспечивал эквивалентное с формотеролом ДПИ улучшение объема форсированного выдоха за 1-ю секунду (площадь под фармакокинетической кривой). При этом эффект Атимоса развивался быстрее, чем у формотерола в ДПИ (5 и 7,5 мин соответственно), и сохранялся в течение 12 ч у большего числа пациентов (51 и 33% соответственно) [11].
Таким образом, преимуществами Атимоса — экстрамелкодисперсного препарата формотерола в виде ДАИ -являются:
• высокая легочная депозиция;
• стабильность доставки независимо от тяжести обструкции и силы вдоха;
• доставка препарата не только в крупные, но и в малые дыхательные пути;
• простота ингаляции и низкий риск ошибок.
Знание врачами всего спектра ингаляционных препаратов, средств доставки и правил проведения ингаляции является необходимым условием эффективности ингаляционной терапии. Большой выбор препаратов и устройств для ингаляционной терапии расширяет возможности их индивидуального подбора для конкретного пациента.
^исок литературы
1. Laube B.L. et al. // Eur.Respir. J. 2011. V. 37. P. 1308.
2. Molimard H.et al. // J. Aerosol Med. 2003. V. 16. P. 249.
3. Lavopini F. et al. // Respir. Med. 2008. V. 102. P. 593.
4. Crampton G.K. et al. // Eur. J. Respir. Dis. 1982. V. 63. P. 101.
5. Melani A.S. et al. // Respir. Med. 2011. V. 105. P. 930.
6. van der Palen J. et al. // Eur. Respir. J. 1999. V. 14. P. 1034.
7. Acerbi D. et al. // Pulm. Pharmacol. Ther. 2007. V. 20. P. 290.
8. Crée C.P. et al. // J. Aerosol Med. 2006. V. 19. P. 466.
9. Meyer T. et al. // J. Aerosol Med. 2004. V. 17. P. 43.
10. Nadarassan D.K. et al. //Eur. J. Pharm. Sei. 2010. V. 39. P. 348.
11. Bousquet J. et al. //Respiration. 2005. V. 72. Suppl. 1. P. 13. .
МОСФЕРА П
atm-press.ru
На сайте atm-press.ru вы сможете ПРИОБРЕСТИ все наши книги и журналы по издательским ценам без магазинных наценок. Также на сайте atm-press.ru В БЕСПЛАТНОМ ДОСТУПЕ вы найдете архив журналов «Атмосфера. Пульмонология и аллергология», «Астма и аллергия’ «Лечебное дело», «Атмосфера. Новости кардиологии», «Нервные болезни», «Нервы», переводы на русский язык руководств и брошюр.
Впечатления от использования этого устройства у пациентов разные. Кому-то небулайзер помог, а кому-то ещё больше усложнил ситуацию. Причиной этого являются ошибки, возникающие из-за неумения многих пользоваться этим ингалятором.
Ошибки при использовании ингалятора
Первая ошибка – использование прибора при любых простудных заболеваниях. Он эффективен только тогда, когда воспалена слизистая гортани или нижние дыхательные пути. В этом случае небулайзер эффективен, так как вылечиться можно, только распылив лекарственное средство на органы дыхательной системы. Поэтому для лечения фарингита и обычного насморка нужен другой вид устройства.
Вторая – самостоятельный подбор лекарства. Самостоятельный отбор отхаркивающего препарата может спровоцировать появление бронхообструкций, стать причиной увеличения количества мокроты. Врачи подбирают лекарство, изучив тип кашля, его мокроту, вязкость и прочее.
Третья ошибка – время выполнения ингаляций. Частота ингаляций назначается врачом в зависимости от сложности заболевания, в среднем три раза за день. Лучше делать ингаляции через час после приема пищи, так как в это время происходит увеличение внутрибрюшного давления и происходит давление органов живота на диафрагму, вследствие чего выполняется уменьшение дыхательного объёма.
Четвертая ошибка – использование небулайзера после другого человека. Многие семьи в средствах экономии делают ингаляции одним прибором по очереди. После каждого использования мундштук, дозатор и маску нужно обрабатывать антисептическим раствором.